

Enhanced T cell recovery in HIV-1-infected adults through IL-7 treatment
- PMID: 19287090
- PMCID: PMC2662568
- DOI: 10.1172/JCI38052
Enhanced T cell recovery in HIV-1-infected adults through IL-7 treatment
Abstract
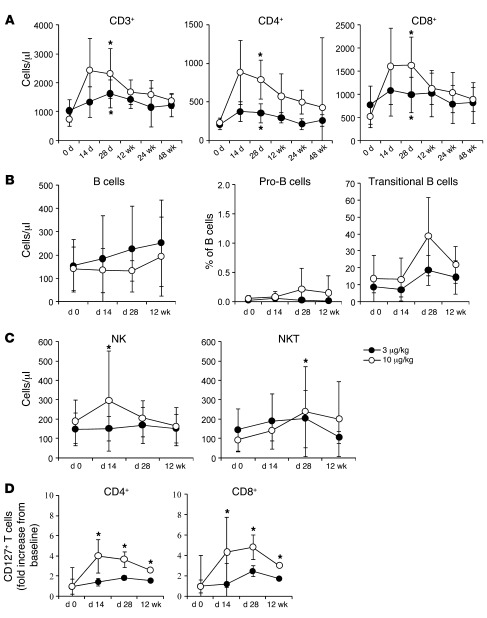
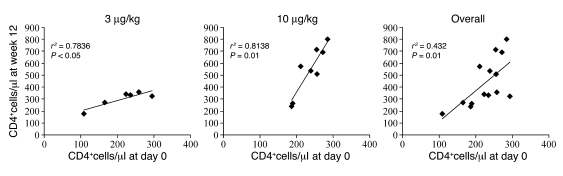
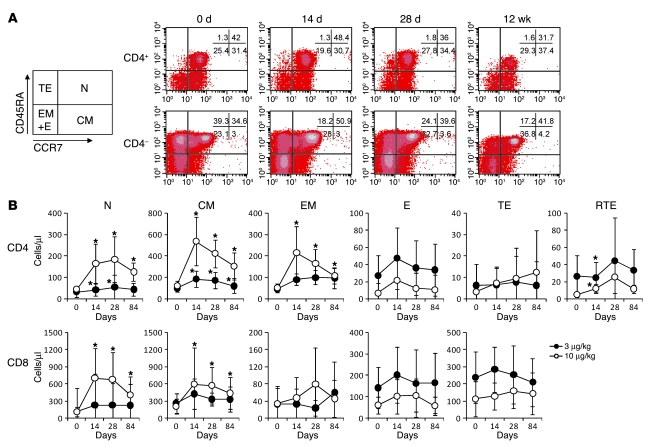
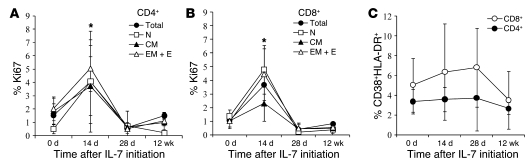
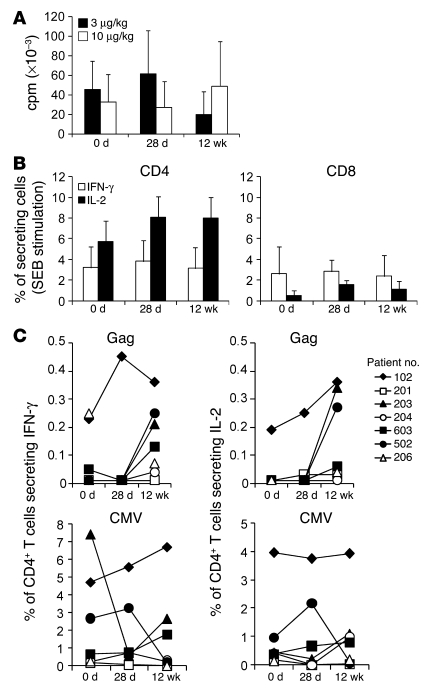
HIV infection results in CD4+ T cell deficiency, but efficient combination antiretroviral therapy (c-ART) restores T cells and decreases morbidity and mortality. However, immune restoration by c-ART remains variable, and prolonged T cell deficiency remains in a substantial proportion of patients. In a prospective open-label phase I/IIa trial, we evaluated the safety and efficacy of administration of the T cell regulator IL-7. The trial included 13 c-ART-treated HIV-infected patients whose CD4+ cell counts were between 100 and 400 cells/microl and plasma HIV RNA levels were less than 50 copies/ml. Patients received a total of 8 subcutaneous injections of 2 different doses of recombinant human IL-7 (rhIL-7; 3 or 10 microg/kg) 3 times per week over a 16-day period. rhIL-7 was well tolerated and induced a sustained increase of naive and central memory CD4+ and CD8+ T cells. In the highest dose group, 4 patients experienced transient increases in viral replication. However, functional assays showed that the expanded T cells responded to HIV antigen by producing IFN-gamma and/or IL-2. In conclusion, in lymphopenic HIV-infected patients, rhIL-7 therapy induced substantial functional and quantitative changes in T cells for 48 weeks. Therefore, patients may benefit from intermittent therapy with IL-7 in combination with c-ART.
Figures
References
-
- Hammer S.M., et al. A controlled trial of two nucleoside analogues plus indinavir in persons with human immunodeficiency virus infection and CD4 cell counts of 200 per cubic millimeter or less. AIDS Clinical Trials Group 320 Study Team. N. Engl. J. Med. 1997;337:725–733. doi: 10.1056/NEJM199709113371101. - DOI - PubMed
-
- Palella F.J., Jr., et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N. Engl. J. Med. 1998;338:853–860. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
