

Protection of the ischaemic heart: investigations into the phenomenon of ischaemic preconditioning
- PMID: 19287816
- PMCID: PMC4200578
Protection of the ischaemic heart: investigations into the phenomenon of ischaemic preconditioning
Abstract
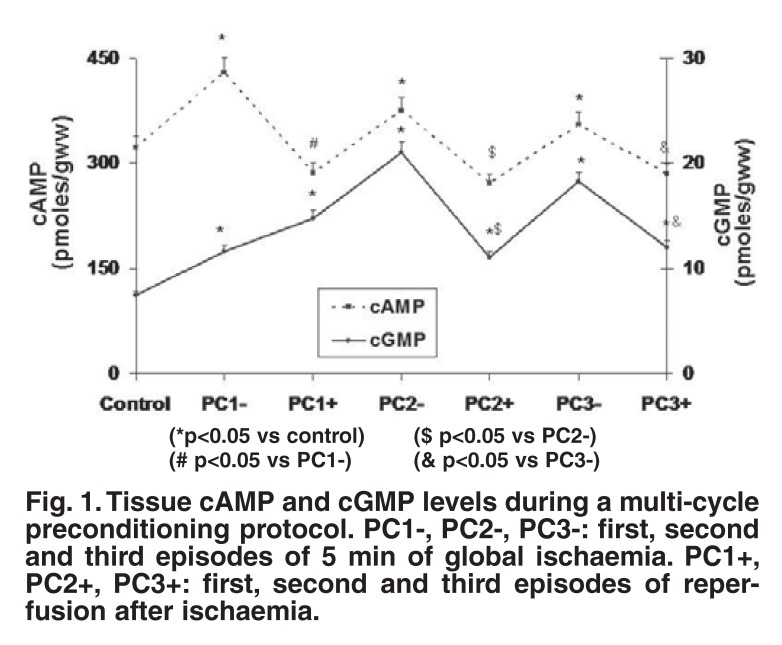
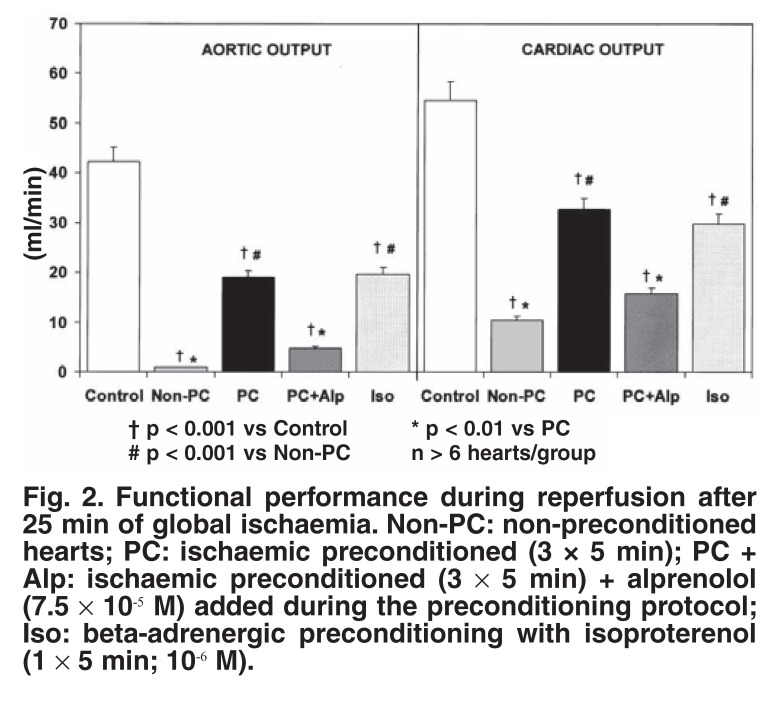
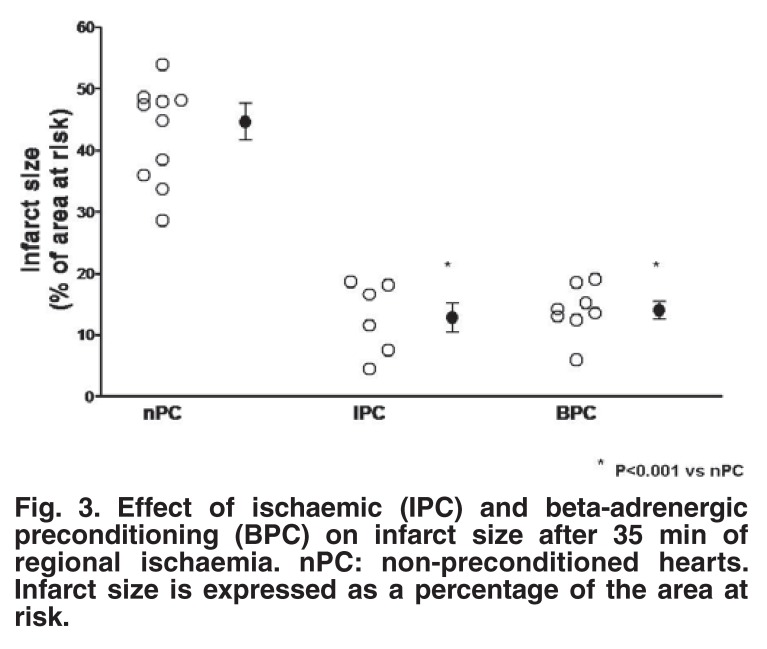
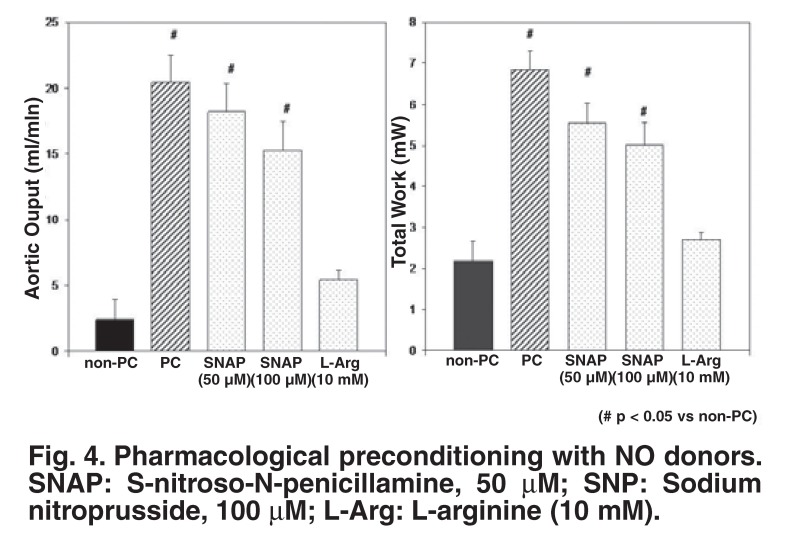
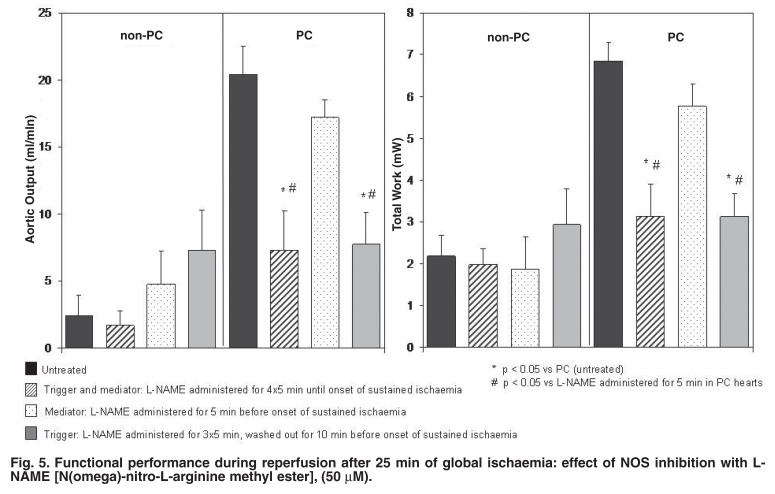
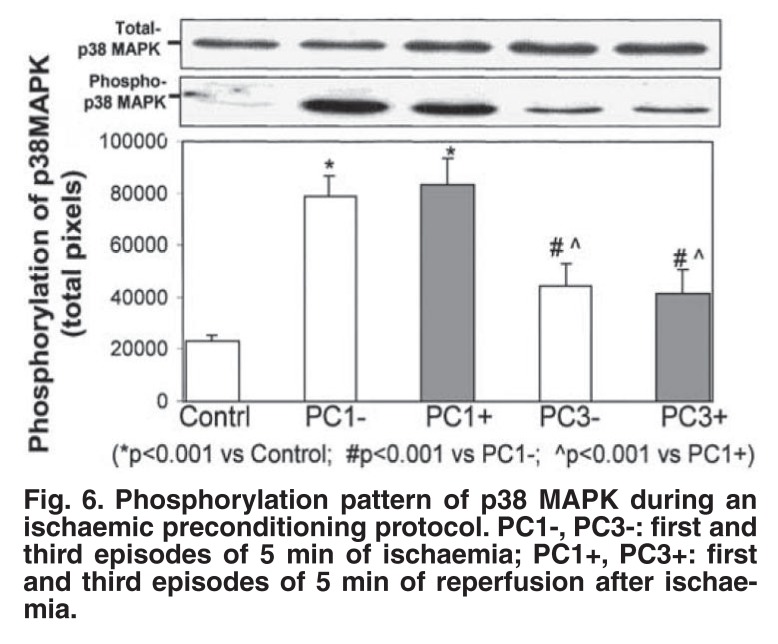
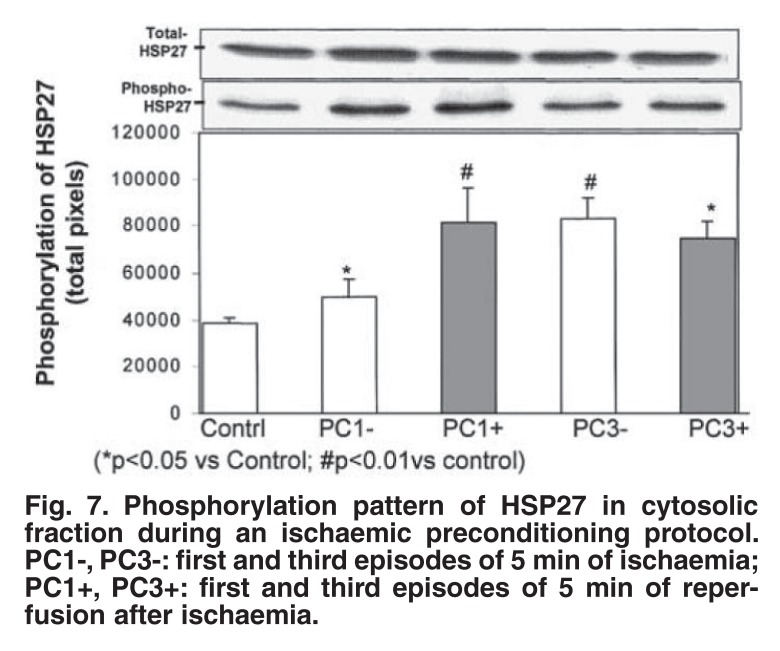
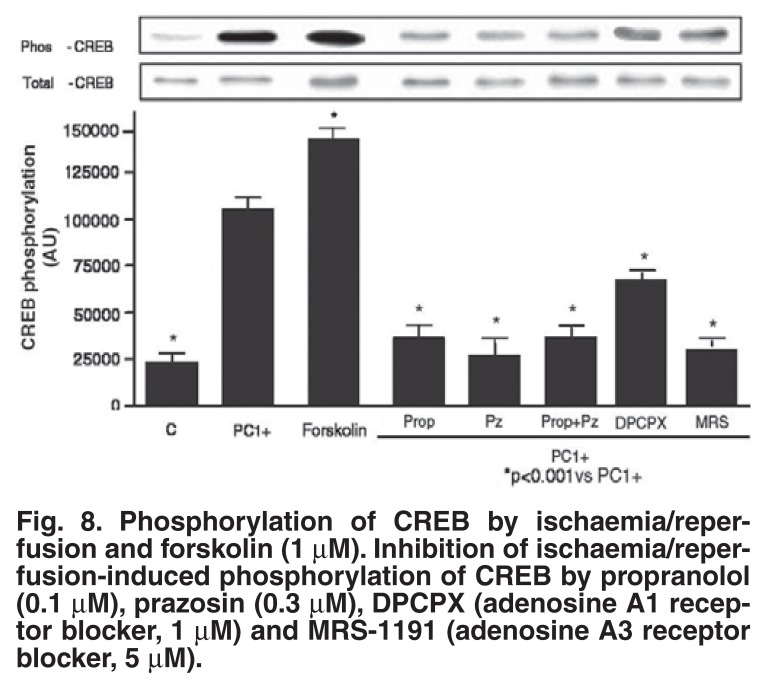
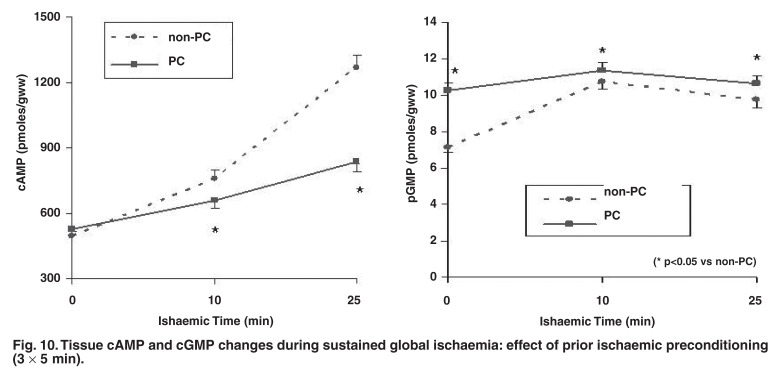
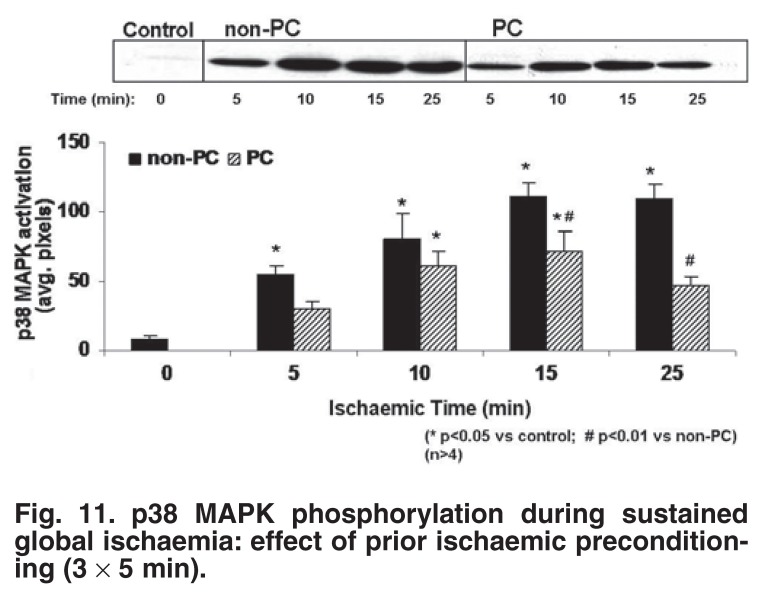
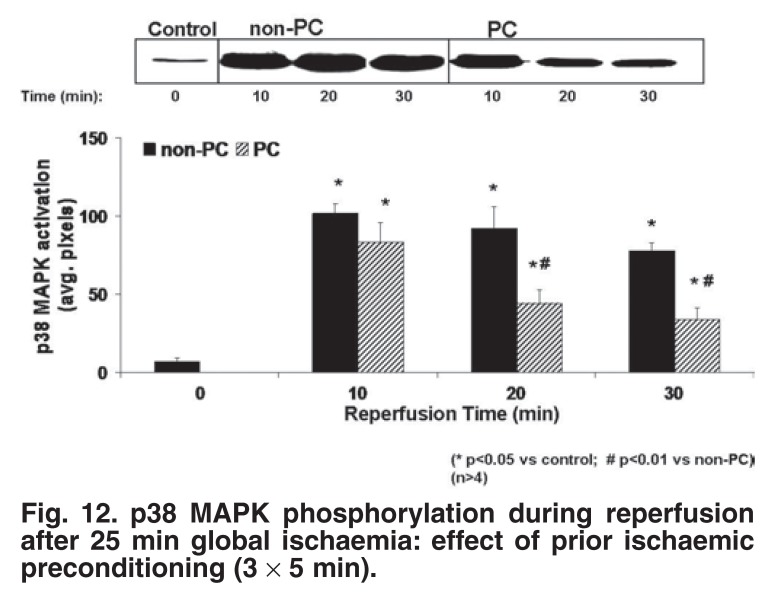
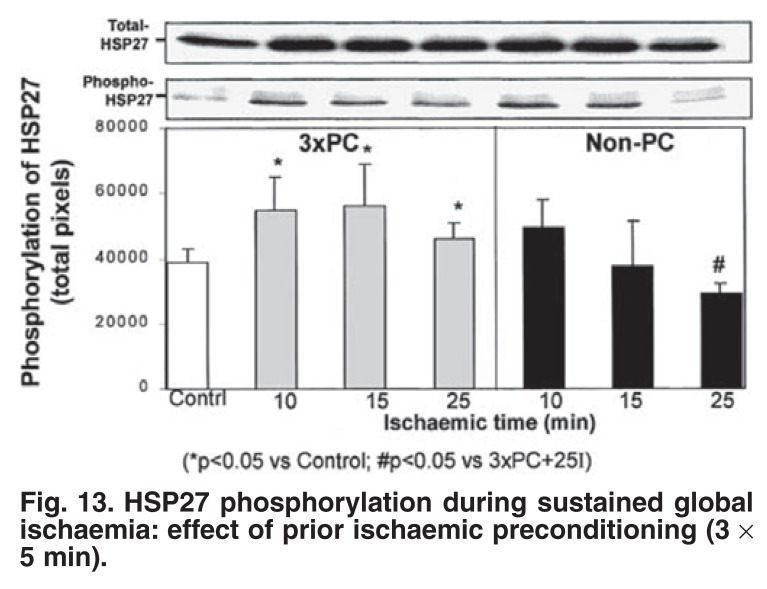
Exposure of the heart to one or more short episodes of ischaemia/reperfusion protects the heart against a subsequent prolonged period of ischaemia, as evidenced by a reduction in infarct size and an improvement in functional recovery during reperfusion. Elucidation of the mechanism of this endogenous protection could lead to the development of pharmacological mimetics to be used in the clinical setting. The aim of our studies was therefore to gain more information regarding the mechanism of ischaemic preconditioning, using the isolated perfused working rat heart as model. A preconditioning protocol of 1 x 5 or 3 x 5 min of ischaemia, interspersed with 5 min of reperfusion was found to protect hearts exposed to 25 min of global ischaemia or 35-45 min of regional ischaemia. These models were used throughout our studies. In view of the release of catecholamines by ischaemic tissue, our first aim was to evaluate the role of the alphaadrenergic receptor in ischaemic preconditioning. However, using a multi-cycle ischaemic preconditioning protocol, we could not find any evidence for alpha-1 adrenergic or PKC activation in the mechanism of preconditioning. Cyclic increases in the tissue cyclic nucleotides, cAMP and cGMP were found, however, to occur during a multi-cycle preconditioning protocol, suggesting roles for the beta-adrenergic signalling pathway and nitric oxide (NO) as triggers of cardioprotection. This was substantiated by the findings that (1) administration of the beta-adrenergic agonist, isoproterenol, or the NO donors SNAP or SNP before sustained ischaemia also elicited cardioprotection similar to ischaemic preconditioning; (2) beta-adrenergic blockade or nitric oxide synthase inhibition during an ischaemic preconditioning protocol abolished protection. Effectors downstream of cAMP, such as p38MAPK and CREB, were also demonstrated to be involved in the triggering process. Our next step was to evaluate intracellular signalling during sustained ischaemia and reperfusion. Our results showed that ischaemic preconditioned-induced cardioprotection was associated with a significant reduction in tissue cAMP, attenuation of p38MAPK activation and increased tissue cGMP levels and HSP27 activation, compared to non-preconditioned hearts. The role of the stress kinase p38MAPK was further investigated by using the inhibitor SB203580. Our results suggested that injury by necrosis and apoptosis share activation of p38MAPK as a common signal transduction pathway and that pharmacological targeting of this kinase offers a tenable option to manipulate both these processes during ischaemia/reperfusion injury.
Figures

References
-
- Murray CJ, Lopez AD. Alternate projections of mortality and disability by cause 1990–2020: global burden of disease study. Lancet. 1997;349:1498–1504. - PubMed
-
- Murry CE, Jennings RB, Reimer KA. Preconditioning with ischemia: a delay of lethal cell injury in ischemic myocardium. Circulation. 1986;74:1124–1136. - PubMed
-
- Kloner RA, Shook T, Entman EM. et al. Prospective temporal analysis of the onset of preinfarction angina versus outcome: an ancillary study in TIMI-9B. Circulation. 1998;97:1042–1045. - PubMed
-
- Yellon DM, Downey JM. Preconditioning the myocardium: from cellular physiology to clinical cardiology. Physiol Rev. 2003;83:1113–1151. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
