

Procalcitonin kinetics within the first days of sepsis: relationship with the appropriateness of antibiotic therapy and the outcome
- PMID: 19291325
- PMCID: PMC2689475
- DOI: 10.1186/cc7751
Procalcitonin kinetics within the first days of sepsis: relationship with the appropriateness of antibiotic therapy and the outcome
Abstract
Introduction: Management of the early stage of sepsis is a critical issue. As part of it, infection control including appropriate antibiotic therapy administration should be prompt. However, microbiological findings, if any, are generally obtained late during the course of the disease. The potential interest of procalcitonin (PCT) as a way to assess the clinical efficacy of the empirical antibiotic therapy was addressed in the present study.
Methods: An observational cohort study including 180 patients with documented sepsis was conducted in our 15-bed medical intensive care unit (ICU). Procalcitonin measurement was obtained daily over a 4-day period following the onset of sepsis (day 1 (D1) to D4). The PCT time course was analyzed according to the appropriateness of the first-line empirical antibiotic therapy as well as according to the patient outcome.
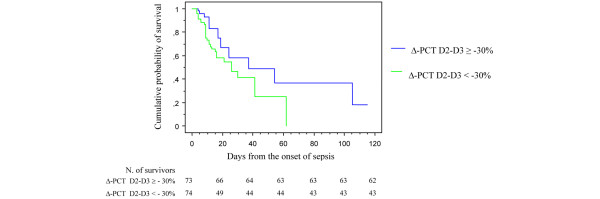
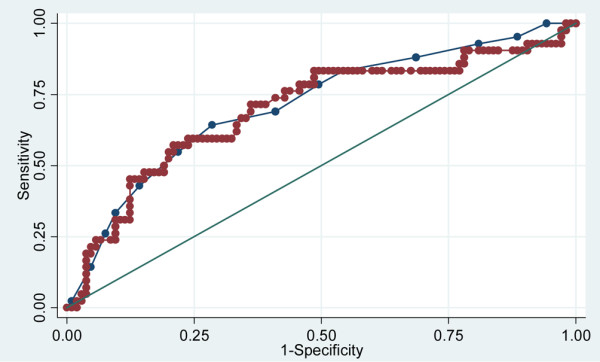
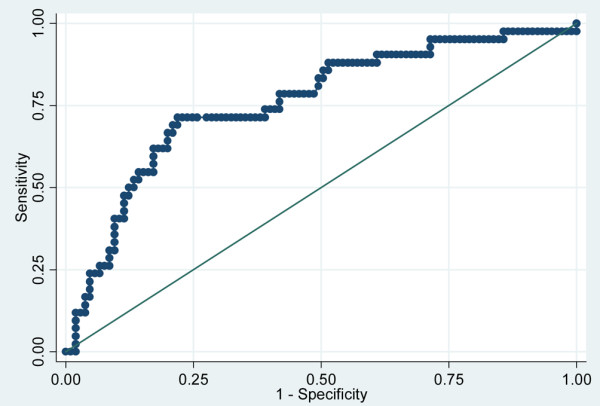
Results: Appropriate first-line empirical antibiotic therapy (n = 135) was associated with a significantly greater decrease in PCT between D2 and D3 (DeltaPCT D2-D3) (-3.9 (35.9) vs. +5.0 (29.7), respectively; P < 0.01). In addition, DeltaPCT D2-D3 was found to be an independent predictor of first-line empirical antibiotic therapy appropriateness. In addition, a trend toward a greater rise in PCT between D1 and D2 was observed in patients with inappropriate antibiotics as compared with those with appropriate therapy (+5.2 (47.4) and +1.7 (35.0), respectively; P = 0.20). The D1 PCT level failed to predict outcome, but higher levels were measured in the nonsurvivors (n = 51) when compared with the survivors (n = 121) as early as D3 (40.8 (85.7) and 21.3 (41.0), respectively; P = 0.04). Moreover, PCT kinetics between D2 and D3 were also found to be significantly different, since a decrease >or= 30% was expected in the survivors (log-rank test, P = 0.04), and was found to be an independent predictor of survival (odds ratio = 2.94; 95% confidence interval 1.22 to 7.09; P = 0.02).
Conclusions: In our study in an ICU, appropriateness of the empirical antibiotic therapy and the overall survival were associated with a greater decline in PCT between D2 and D3. Further studies are needed to assess the utility of the daily monitoring of PCT in addition to clinical evaluation during the early management of sepsis.
Figures
References
-
- Garrouste-Orgeas M, Timsit JF, Tafflet M, Misset B, Zahar JR, Soufir L, Lazard T, Jamali S, Mourvillier B, Cohen Y, De Lassence A, Azoulay E, Cheval C, Descorps-Declere A, Adrie C, Costa de Beauregard MA, Carlet J. Excess risk of death from intensive care unit-acquired nosocomial bloodstream infections: A reappraisal. Clin Infect Dis. 2006;42:1118–1126. doi: 10.1086/500318. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
