

The phenotype of persons having mosaicism for trisomy 21/Down syndrome reflects the percentage of trisomic cells present in different tissues
- PMID: 19291777
- PMCID: PMC3707311
- DOI: 10.1002/ajmg.a.32729
The phenotype of persons having mosaicism for trisomy 21/Down syndrome reflects the percentage of trisomic cells present in different tissues
Abstract
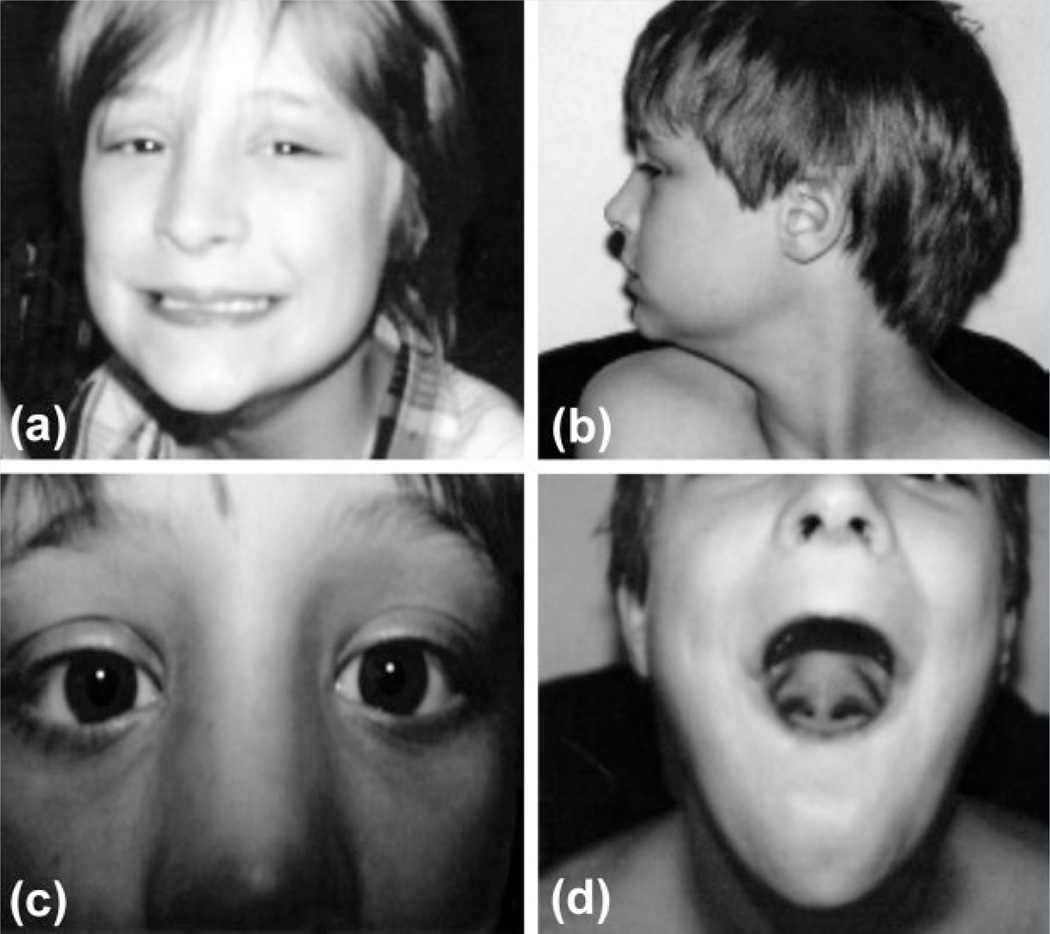
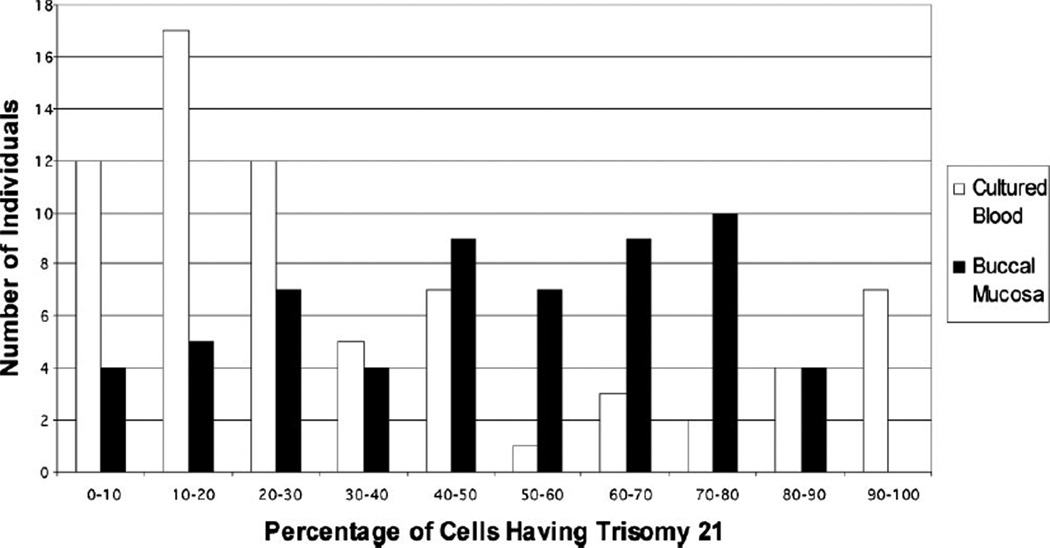
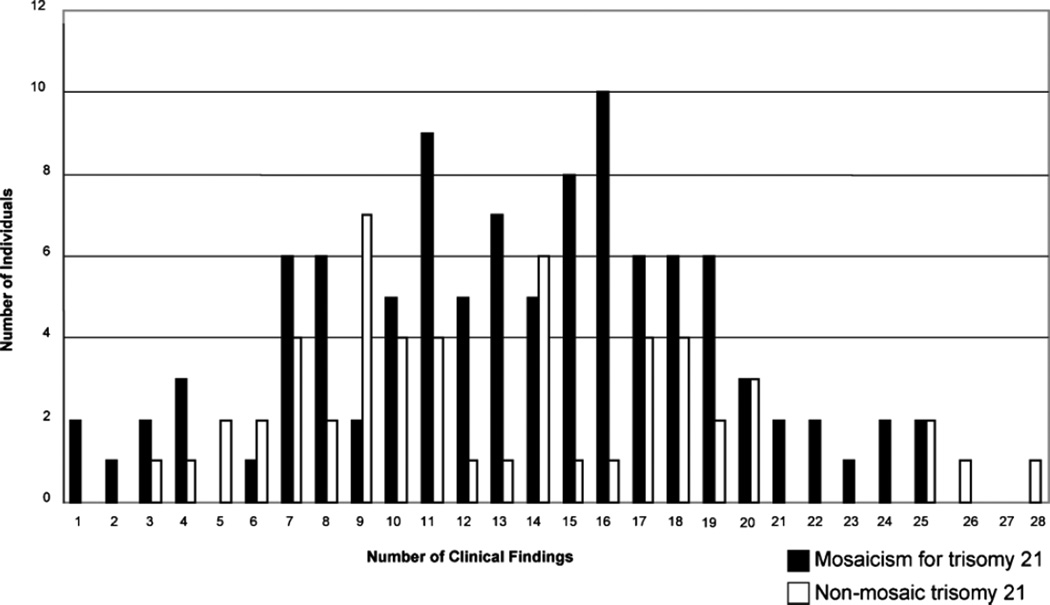
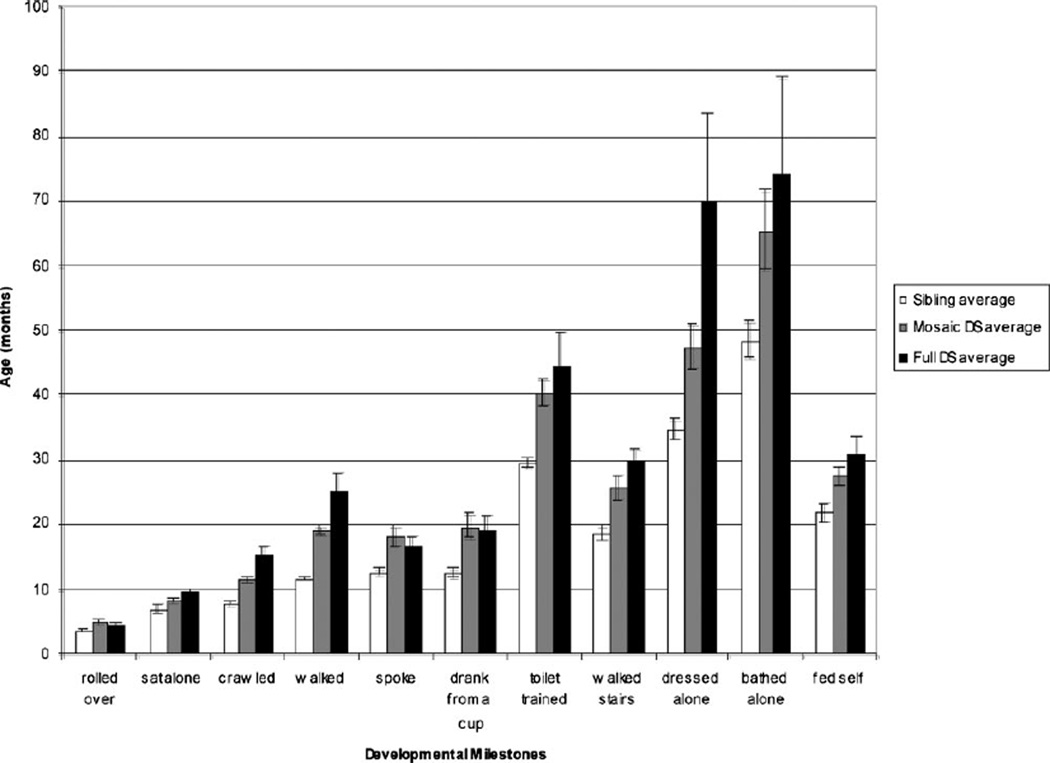
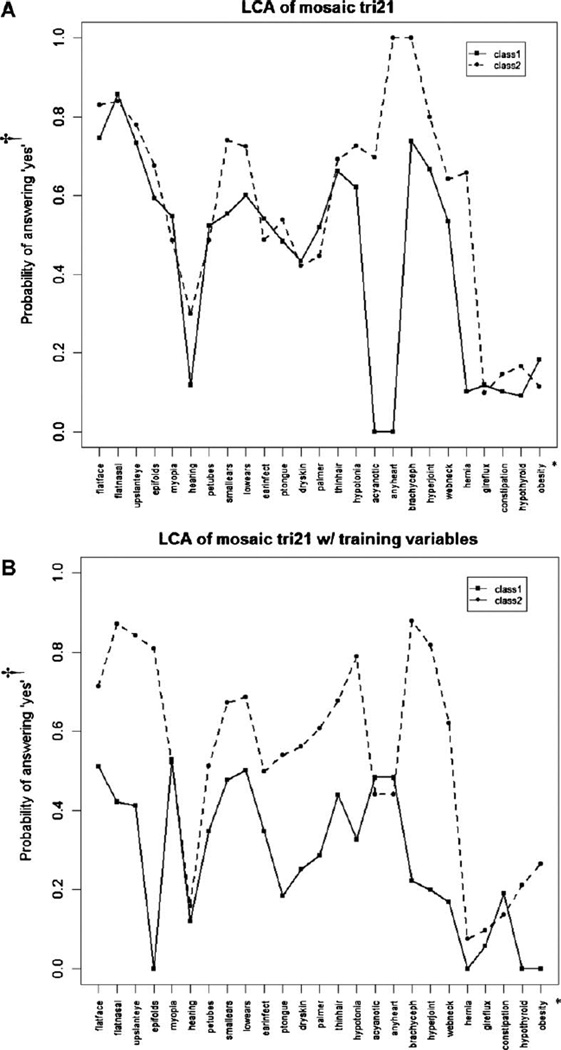
Little is known about the pathogenesis of the phenotype in individuals with trisomy 21 mosaicism and Down syndrome. The primary goal of this study was to identify factors contributing to the observed phenotypic variation by evaluating 107 individuals having trisomy 21 mosaicism. To investigate a potential "threshold" effect due to trisomic imbalance, lymphocyte and buccal mucosa nuclei were scored using FISH. Overall, buccal cells showed a significantly higher frequency of trisomy than lymphocytes (P < 0.0001). Using latent class analysis, two phenotypic classes were identified based on the clinical findings of the propositi. Patients from class 1 had significantly fewer traits and a lower percentage of trisomic cells (mean of 37.3% lymphocytes; 34.5% buccal mucosa cells) when compared to those stratified into class 2 (54.0% lymphocytes; 53.4% buccal mucosa cells). Tissue-specific influences were also detected, with buccal mucosa trisomy levels being significantly correlated with IQ (P = 0.0094; both ectodermal derivatives), while congenital heart defects were significantly correlated with lymphocytes (P = 0.0286; both mesodermal embryonic derivatives). In conclusion, allowing for the distinction of two groups, we observed variation in phenotype, associated with the percentage of trisomic cells. We also observed tissue-specific effects on phenotype. The results of this study should enable geneticists and other health care professionals to provide information regarding optimal diagnostic approaches and anticipated clinical outcomes.
Figures
References
-
- Alvares O, Skougaard MR, Pindborg JJ, Roed-Petersen B. In vitro incorporation of tritiated thymidine in oral homogeneous leukoplakias. Scand J Dent Res. 1972;80:510–514. - PubMed
-
- Bhatt S, Schreck R, Graham JM, Korenberg JR, Hurvitz CG, Fischel-Ghodsian N. Transient leukemia with trisomy 21: Description of a case and review of the literature. Am J Med Genet. 1995;58:310–314. - PubMed
-
- Dewald G, Stallard R, Al Saadi A, Arnold S, Bader PI, Blough R, Chen K, Elejalde BR, Harris CJ, Higgins RR, Hoeltge GA, Hsu W-T, Kubic V, McCorquodale DJ, Micale MA, Moore JW, Phillips RM, Scheib-Wixted S, Schwartz S, Siembieda S, Strole K, VanTuinen P, Vance GH, Wiktor A, Wise L, Yung J-F, Zenger-Hain J, Zinsmeister A. A multi-center investigation with interphase in situ hybridization using X- and Y-chromosome probes. Am J Med Genet. 1998;76:318–326. - PubMed
-
- Epstein CJ, Korenberg JR, Anneren G, Antonarakis SE, Ayme S, Courchesne E, Epstein LB, Fowler A, Groner Y, Huret JL, Kempler TL, Lott IT, Lubin BH, Magenis E, Opitz J, Patterson D, Priets JH, Pueschel SM, Rapoport SI, Sinet PM, Tanzi RE, de la Cruz F. Protocols to establish genotype-phenotype correlations in Down syndrome. Am J Med Genet. 1991;49:207–235. - PMC - PubMed
-
- Finley WH, Finley SC, Rosecrans CJ, Tucker CC. Normal/trisomy 21 mosaicism. Report of four cases and review of the subject. Am J Dis Child. 1966;112:444–447. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
