

Gender is an age-specific effect modifier for papillary cancers of the thyroid gland
- PMID: 19293311
- PMCID: PMC2667567
- DOI: 10.1158/1055-9965.EPI-08-0976
Gender is an age-specific effect modifier for papillary cancers of the thyroid gland
Abstract
Background: Thyroid cancer incidence rates have increased worldwide for decades, although more for papillary carcinomas than other types and more for females than males. There are few known thyroid cancer risk factors except female gender, and the reasons for the increasing incidence and gender differences are unknown.
Methods: We used the National Cancer Institute's Surveillance, Epidemiology, and End Results 9 Registries Database for cases diagnosed during 1976-2005 to develop etiological clues regarding gender-related differences in papillary thyroid cancer incidence. Standard descriptive epidemiology was supplemented with age-period-cohort (APC) models, simultaneously adjusted for age, calendar-period and birth-cohort effects.
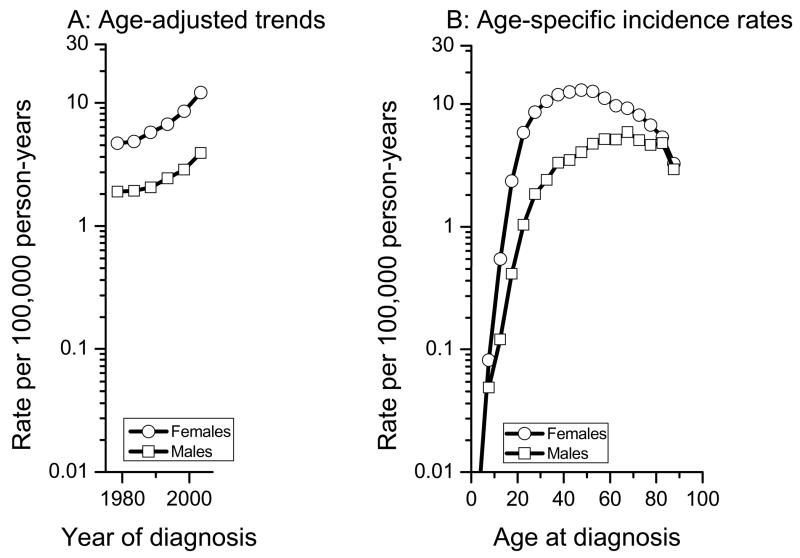
Results: The papillary thyroid cancer incidence rate among females was 2.6 times that among males (9.2 versus 3.6 per 100,000 person-years, respectively), with a widening gender gap over time. Age-specific rates were higher among women than men across all age groups, and the female-to-male rate ratio declined quite consistently from more than five at ages 20-24 to 3.4 at ages 35-44 and approached one at ages 80+. APC models for papillary thyroid cancers confirmed statistically different age-specific effects among women and men (P < 0.001 for the null hypothesis of no difference by gender), adjusted for calendar-period and birth-cohort effects.
Conclusion: Gender was an age-specific effect modifier for papillary thyroid cancer incidence. Future analytic studies attempting to identify the risk factors responsible for rising papillary thyroid cancer incidence should be designed with adequate power to assess this age-specific interaction among females and males.
Conflict of interest statement
None of the co-authors has a financial conflict of interest that would have affected this research. This research was supported in part by the Intramural Research Program of the National Institutes of Health, National Cancer Institute. The authors had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Figures



References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008 Mar-Apr;58(2):71–96. Epub 2008 Feb 20. - PubMed
-
- Zheng T, Holford TR, Chen Y, et al. Time trend and age-period-cohort effect on incidence of thyroid cancer in Connecticut, 1935–1992. Int J Cancer. 1996 Aug 7;67(4):504–509. - PubMed
-
- Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973–2002. JAMA. 2006 May 10;295(18):2164–2167. - PubMed
-
- Reynolds RM, Weir J, Stockton DL, Brewster DH, Sandeep TC, Strachan MW. Changing trends in incidence and mortality of thyroid cancer in Scotland. Clin Endocrinol (Oxf) 2005 Feb;62(2):156–162. - PubMed
-
- Albores-Saavedra J, Henson DE, Glazer E, Schwartz AM. Changing patterns in the incidence and survival of thyroid cancer with follicular phenotype--papillary, follicular, and anaplastic: a morphological and epidemiological study. Endocr Pathol. 2007 Spring;18(1):1–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
