

Characterization of a preclinical model of chronic ischemic wound
- PMID: 19293328
- PMCID: PMC2685508
- DOI: 10.1152/physiolgenomics.90362.2008
Characterization of a preclinical model of chronic ischemic wound
Abstract
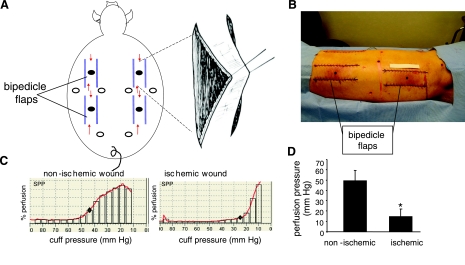
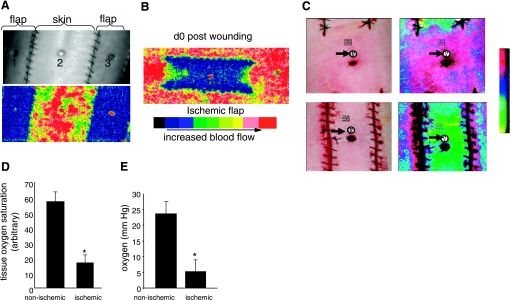
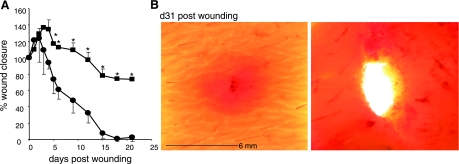
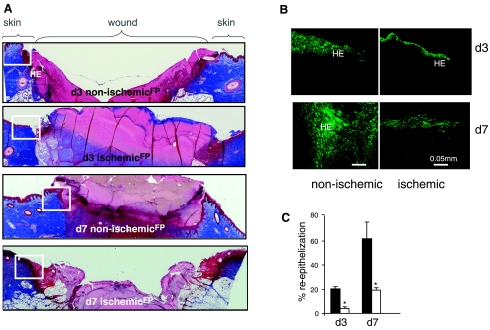
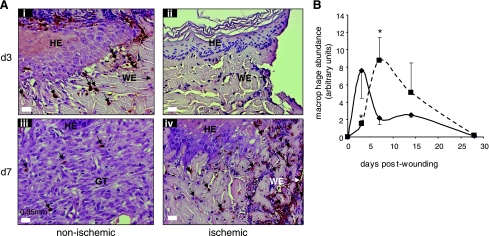
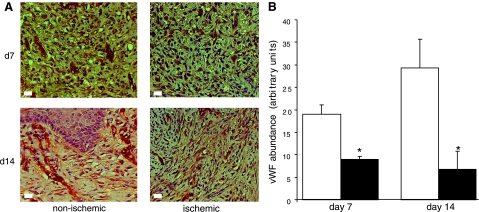
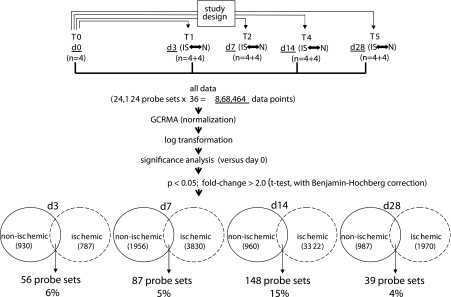
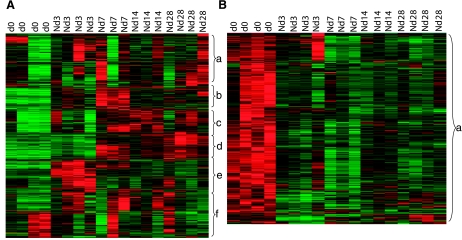
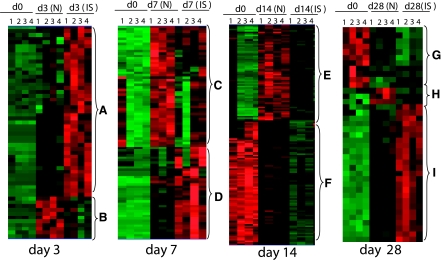
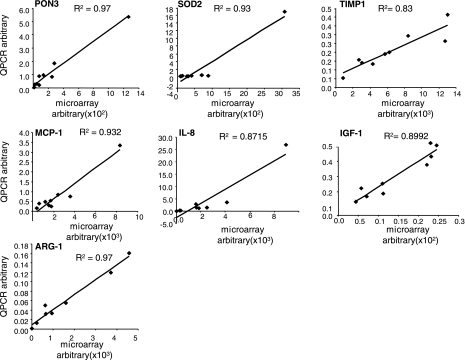
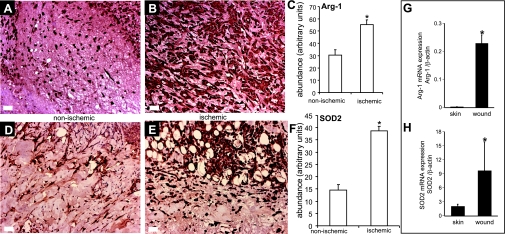
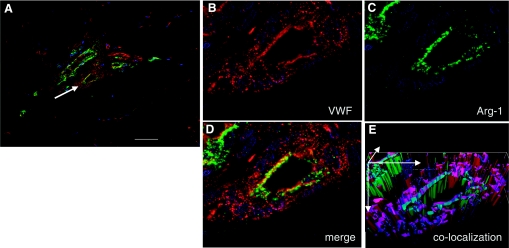
Chronic ischemic wounds presenting at wound clinics are heterogeneous with respect to etiology, age of the wound, and other factors complicating wound healing. In addition, there are ethical challenges associated with collecting repeated biopsies from a patient to develop an understanding of the temporal dynamics of the mechanisms underlying chronic wounds. The need for a preclinical model of ischemic wound is therefore compelling. The porcine model is widely accepted as an excellent preclinical model for human wounds. A full-thickness bipedicle flap approach was adopted to cause skin ischemia. Closure of excisional wounds placed on ischemic tissue was severely impaired resulting in chronic wounds. Histologically, ischemic wounds suffered from impaired re-epithelialization, delayed macrophage recruitment and poorer endothelial cell abundance and organization. Compared with the pair-matched nonischemic wound, unique aspects of the ischemic wound biology were examined on days 3, 7, 14, and 28 by systematic screening of the wound tissue transcriptome using high-density porcine GeneChips. Ischemia markedly potentiated the expression of arginase-1, a cytosolic enzyme that metabolizes the precursor of nitric oxide l-arginine. Ischemia also induced the SOD2 in the wound tissue perhaps as survival response of the challenged tissue. Human chronic wounds also demonstrated elevated expression of SOD2 and arginase-1. This study provides a thorough database that may serve as a valuable reference tool to develop novel hypotheses aiming to elucidate the biology of ischemic chronic wounds in a preclinical setting.
Figures
References
-
- Abd-El-Aleem SA, Ferguson MW, Appleton I, Kairsingh S, Jude EB, Jones K, McCollum CN, Ireland GW. Expression of nitric oxide synthase isoforms and arginase in normal human skin and chronic venous leg ulcers. J Pathol 191: 434–442, 2000. - PubMed
-
- Becker F, Raoux MH, Brenot R, David M. Predictive value of TcPO2 in chronical severe ischemia of lower limbs. Int J Microcir Clin Exp 7: 261–271, 1988.
-
- Bernatchez SF, Parks PJ, Grussing DM, Matalas SL, Nelson GS. Histological characterization of a delayed wound healing model in pig. Wound Repair Regen 6: 223–233, 1998. - PubMed
-
- Broughton G 2nd, Janis JE, Attinger CE. The basic science of wound healing. Plast Reconstr Surg 117: 12S–34S, 2006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials