

Insights into endometrial serous carcinogenesis and progression
- PMID: 19294001
- PMCID: PMC2655156
Insights into endometrial serous carcinogenesis and progression
Abstract
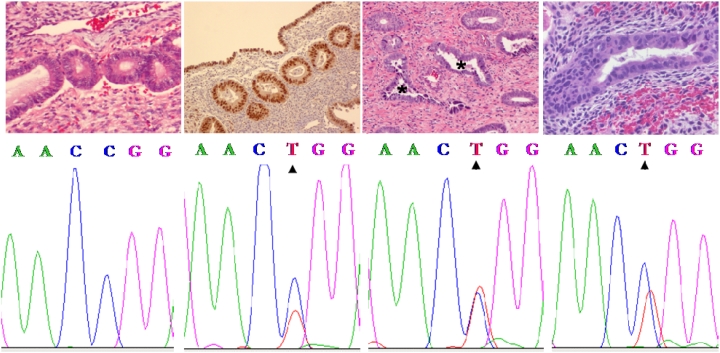
Endometrial serous carcinomas (ESC) constitute only approximately 10% of endometrial cancers, but have a substantially higher case-fatality rate than their more common endometrioid counterparts. The precise composite of factors driving endometrial serous carcinogenesis and progression remain largely unknown, but we attempt to review the current state of knowledge in this report. ESC probably do not evolve through a single pathway, and their underlying molecular events probably occur early in their evolution. TP53 gene mutations occur in 22.7 to 96% of cases, and p53 protein overexpression is seen in approximately 76%. By gene expression profiling, p16 is upregulated in ESC significantly above both normal endometrial cells and endometrioid carcinomas, and 92-100% of cases display diffuse expression of the p16 protein by immunohistochemistry (IHC). Together, these findings suggest dysregulation of both the p16(INKA)/Cyclin D-CDK/pRb-E2F and the ARF-MDM2-p53 cell cycle pathways in ESC. By IHC, HER2/neu is overexpressed (2+ or 3+) in approximately 32.1% of ESC, and approximately 54.5% of cases scored as 2+ or 3+ by IHC display c-erbB2 gene amplification as assessed by fluorescent in situ hybridization. Genetic instability, typically manifested as loss of heterozygosity in multiple chromosomes, is a common feature of ESC, and one study found loss of heterozygosity at 1p32-33 in 63% of cases. A subset of ESC display protein expression patterns that are characteristic of high grade endometrial carcinomas, including loss of the metastasis suppressor CD82 (KAI-1) and epithelial-to-mesenchymal transformation, the latter manifested as E-cadherin downregulation, P-cadherin upregulation, and expression of epithelial-to-mesenchymal transformation-related molecules such as zinc-finger E-box-binding homeobox 1 (ZEB1) and focal adhesion kinase. Preliminary data suggests differential patterns of expression in ESC of some isoforms of claudins, proteases, the tumor invasiveness and progression-associated oncofetal protein insulin-like growth factor II mRNA-binding protein 3 (IMP3), as well as a variety of other molecules. At the morphologic level, evidence that indicates that endometrial glandular dysplasia (EmGD) is the most likely morphologically recognizable precursor lesion to ESC is presented. We advocate use of the term endometrial intraepithelial carcinoma (EIC, or its other appellations) only as a morphologic descriptor and never as a diagnostic/pathologic statement of biologic potential. Given its potential for extrauterine extension, we consider the lesions described as EIC, when present in isolation, as examples of localized ESC, and patients should be managed as such. Morphologically normal, p53 immunoreactive endometrial cells (the so-called "p53 signatures"), show a statistically significant association with ESC, display p53 mutations in a significant subset, and form the start of a progression model, outlined herein, from p53 signatures to EmGD to localized ESC to the more conventionally invasive neoplasm. The identification of a morphologically-recognizable precursor holds the promise of early detection of ESC, with the attendant reduction in its overall associated mortality rate. Deciphering the molecular basis for endometrial serous carcinogenesis should uncover potential targets for diagnosis, therapy, and/or disease surveillance.
Keywords: CDKs; Endometrial serous carcinoma; MDM2 and HER2/neu (erb-B2); cadherins; claudins; endometrial glandular dysplasia; endometrial intraepithelial carcinoma; p53.
Figures
Similar articles
-
Endometrial glandular dysplasia: a newly defined precursor lesion of uterine papillary serous carcinoma. Part I: morphologic features.Int J Surg Pathol. 2004 Jul;12(3):207-23. doi: 10.1177/106689690401200302. Int J Surg Pathol. 2004. PMID: 15306933
-
Endometrial glandular dysplasia with frequent p53 gene mutation: a genetic evidence supporting its precancer nature for endometrial serous carcinoma.Clin Cancer Res. 2008 Apr 15;14(8):2263-9. doi: 10.1158/1078-0432.CCR-07-4837. Epub 2008 Mar 27. Clin Cancer Res. 2008. PMID: 18369088
-
Endometrial glandular dysplasia: a putative precursor lesion of uterine papillary serous carcinoma. Part II: molecular features.Int J Surg Pathol. 2004 Oct;12(4):319-31. doi: 10.1177/106689690401200405. Int J Surg Pathol. 2004. PMID: 15494858
-
A proposed model for endometrial serous carcinogenesis.Am J Surg Pathol. 2011 Jan;35(1):e1-e14. doi: 10.1097/PAS.0b013e318202772e. Am J Surg Pathol. 2011. PMID: 21164282 Review.
-
[Dualistic model of molecular pathogenesis in endometrial carcinoma].Zentralbl Gynakol. 2002 Jan;124(1):10-6. doi: 10.1055/s-2002-20303. Zentralbl Gynakol. 2002. PMID: 11873308 Review. German.
Cited by
-
Association of insulin-like growth factor II mrna-binding protein 3 (IMP3) expression with prognostic and morphological factors in endometrial cancer.Rev Bras Ginecol Obstet. 2024 Jul 26;46:e-rbgo61. doi: 10.61622/rbgo/2024rbgo61. eCollection 2024. Rev Bras Ginecol Obstet. 2024. PMID: 39176196 Free PMC article.
-
Type II endometrial cancers: A case series.J Midlife Health. 2016 Apr-Jun;7(2):69-72. doi: 10.4103/0976-7800.185335. J Midlife Health. 2016. PMID: 27499593 Free PMC article.
-
[p53 suppresses type II endometrial carcinomas in mice and governs endometrial tumor aggressiveness in humans].Pathologe. 2013 Nov;34 Suppl 2:180-8. doi: 10.1007/s00292-013-1859-x. Pathologe. 2013. PMID: 24196610 German.
-
p53 aberrations in low grade endometrioid carcinoma of the endometrium with nodal metastases: possible insights on pathogenesis discerned from immunohistochemistry.Diagn Pathol. 2017 Nov 14;12(1):81. doi: 10.1186/s13000-017-0668-6. Diagn Pathol. 2017. PMID: 29137657 Free PMC article.
-
Histopathologic diagnosis of endometrial precancers: Updates and future directions.Semin Diagn Pathol. 2022 May;39(3):137-147. doi: 10.1053/j.semdp.2021.12.001. Epub 2021 Dec 10. Semin Diagn Pathol. 2022. PMID: 34920905 Free PMC article. Review.
References
-
- Karpas CM, Bridge MF. Endometrial Adenocarcinoma with Psammomatous Bodies. Am J Obstet Gynecol. 1963;87:935–941. - PubMed
-
- Factor SM. Papillary adenocarcinoma of the endometrium with psammoma bodies. Arch Pathol. 1974;98:201–205. - PubMed
-
- Hameed K, Morgan DA. Papillary adenocarcinoma of endometrium with psammoma bodies. Histology and fine structure. Cancer. 1972;29:1326–1335. - PubMed
-
- LiVolsi VA. Adenocarcinoma of the endometrium with psammoma bodies. Obstet Gynecol. 1977;50:725–728. - PubMed
-
- Cefis F, Carinelli SG, Marzi MM, Senzani F. Endometrial adenocarcinoma with psammoma bodies. Tumori. 1979;65:359–362. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous