

Airway dilator muscle activity and lung volume during stable breathing in obstructive sleep apnea
- PMID: 19294956
- PMCID: PMC2647790
- DOI: 10.1093/sleep/32.3.361
Airway dilator muscle activity and lung volume during stable breathing in obstructive sleep apnea
Abstract
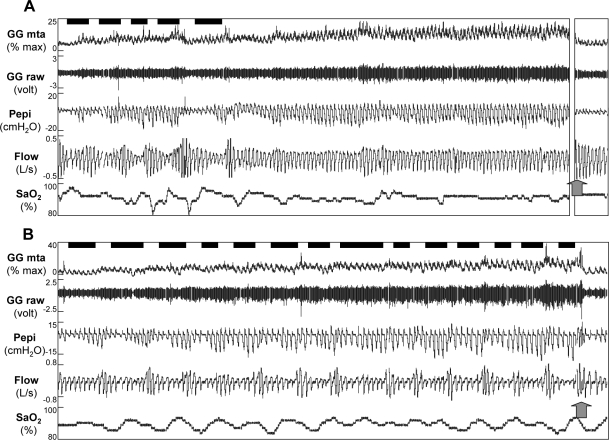
Study objectives: Many patients with obstructive sleep apnea (OSA) have spontaneous periods of stable flow limited breathing during sleep without respiratory events or arousals. In addition, OSA is often more severe during REM than NREM and more severe during stage 2 than slow wave sleep (SWS). The physiological mechanisms for these observations are unknown. Thus we aimed to determine whether the activity of two upper airway dilator muscles (genioglossus and tensor palatini) or end-expiratory lung volume (EELV) differ between (1) spontaneously occurring stable and cyclical breathing and (2) different sleep stages in OSA.
Design: Physiologic observation.
Setting: Sleep physiology laboratory.
Study participants: 15 OSA patients with documented periods of spontaneous stable breathing.
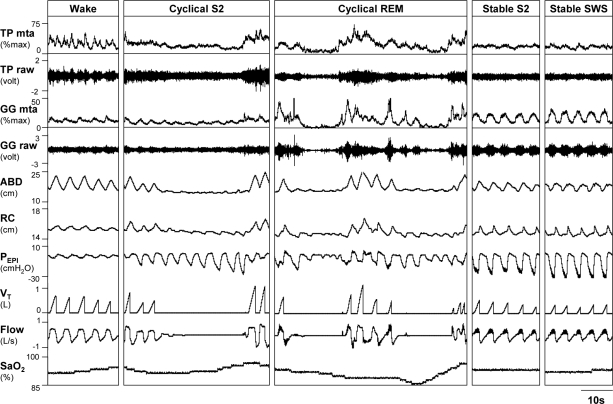
Intervention: Subjects were instrumented with intramuscular electrodes for genioglossus and tensor palatini electromyograms (EMG(GG) and EMG(TP)), chest and abdominal magnetometers (EELV measurement), an epiglottic pressure catheter (respiratory effort), and a mask and pneumotachograph (airflow/ventilation). Patients slept supine overnight without CPAP.
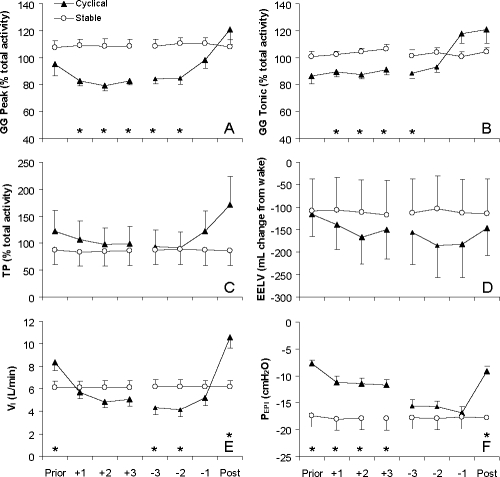
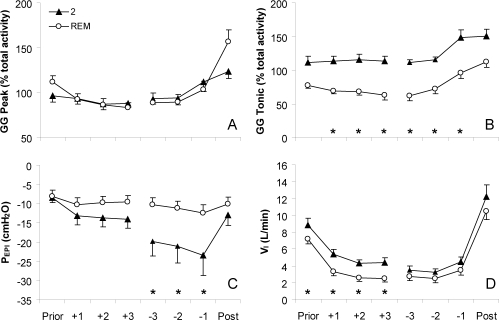
Measurements and results: Peak and Tonic EMG(GG) were significantly lower during cyclical (85.4 +/- 2.7 and 94.6 +/- 4.7 % total activity) than stable breathing (109.4 +/- 0.4 and 103 +/- 0.8% total activity, respectively). During respiratory events in REM, tonic EMG(GG) activity was lower than during respiratory events in stage 2 (71.9 +/- 5.1 and 119.6 +/- 5.6% total activity). EMG(GG) did not differ between stable stage 2 and stable SWS (98.9 +/- 3.2 versus 109.7 +/- 4.4% total activity), nor did EMG(TP) or EELV differ in any breathing condition/sleep stage.
Conclusions: Increased genioglossus muscle tone is associated with spontaneous periods of stable flow limited breathing in the OSA subjects studied. Reductions in genioglossus activity during REM may explain the higher severity of OSA in that stage. Increased lung volume and tensor palatini activity do not appear to be major mechanisms enabling spontaneous stable flow limited breathing periods.
Figures
References
-
- Young T, Blustein J, Finn L, Palta M. Sleep-disordered breathing and motor vehicle accidents in a population- based sample of employed adults. Sleep. 1997;20:608–13. - PubMed
-
- Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378–84. - PubMed
-
- Shahar E, Whitney CW, Redline S, et al. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med. 2001;163:19–25. - PubMed
-
- Stanchina ML, Malhotra A, Fogel RB, et al. Genioglossus muscle responsiveness to chemical and mechanical stimuli during non-rapid eye movement sleep. Am J Respir Crit Care Med. 2002;165:945–9. - PubMed
