

Racial disparities in HIV virologic failure: do missed visits matter?
- PMID: 19295340
- PMCID: PMC2766510
- DOI: 10.1097/QAI.0b013e31818d5c37
Racial disparities in HIV virologic failure: do missed visits matter?
Abstract
Background: Racial/ethnic health care disparities are well described in people living with HIV/AIDS, although the processes underlying observed disparities are not well elucidated.
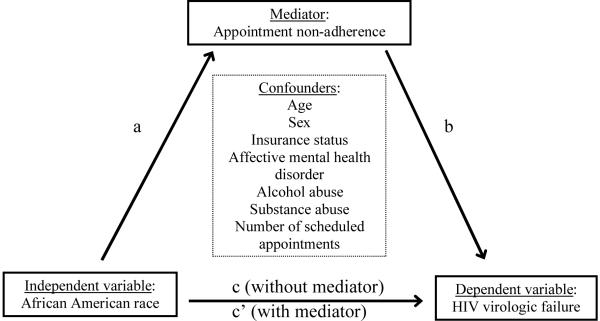
Methods: A retrospective analysis nested in the University of Alabama at Birmingham 1917 Clinic Cohort observational HIV study evaluated patients between August 2004 and January 2007. Factors associated with appointment nonadherence, a proportion of missed outpatient visits, were evaluated. Next, the role of appointment nonadherence in explaining the relationship between African American race and virologic failure (plasma HIV RNA >50 copies/mL) was examined using a staged multivariable modeling approach.
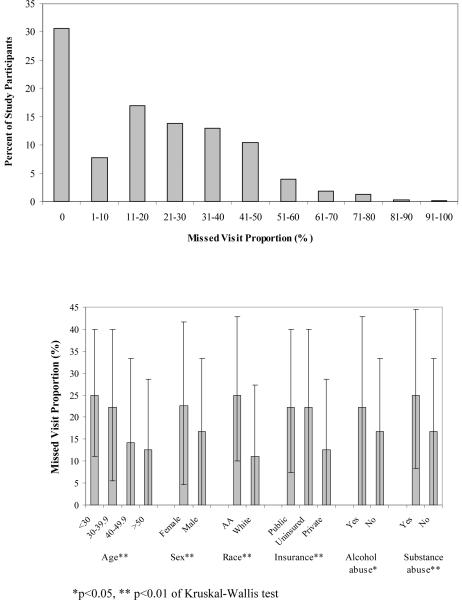
Results: Among 1221 participants, a broad distribution of appointment nonadherence was observed, with 40% of patients missing at least 1 in every 4 scheduled visits. The adjusted odds of appointment nonadherence were 1.85 times higher in African American patients compared with whites [95% confidence interval (CI) = 1.61 to 2.14]. Appointment nonadherence was associated with virologic failure (odds ratio = 1.78, 95% CI = 1.48 to 2.13) and partially mediated the relationship between African American race and virologic failure. African Americans had 1.56 times the adjusted odds of virologic failure (95% CI = 1.19 to 2.05), which declined to 1.30 (95% CI = 0.98 to 1.72) when controlling for appointment nonadherence, a hypothesized mediator.
Conclusions: Appointment nonadherence was more common in African American patients, associated with virologic failure, and seemed to explain part of observed racial disparities in virologic failure.
Figures
References
-
- Shapiro MF, Morton SC, McCaffrey DF, et al. Variations in the care of HIV-infected adults in the United States: results from the HIV Cost and Services Utilization Study. Jama. 1999 Jun 23–30;281(24):2305–2315. - PubMed
-
- Stone VE. Optimizing the care of minority patients with HIV/AIDS. Clin Infect Dis. 2004 Feb 1;38(3):400–404. - PubMed
-
- Betancourt JR. Eliminating racial and ethnic disparities in health care: what is the role of academic medicine? Acad Med. 2006 Sep;81(9):788–792. - PubMed
-
- Lurie N. Health disparities--less talk, more action. N Engl J Med. 2005 Aug 18;353(7):727–729. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
