

Rotator cuff tear pain and tear size and scapulohumeral rhythm
- PMID: 19295959
- PMCID: PMC2657030
- DOI: 10.4085/1062-6050-44.2.148
Rotator cuff tear pain and tear size and scapulohumeral rhythm
Abstract
Context: The body of knowledge concerning shoulder kinematics in patients with rotator cuff tears is increasing. However, the level of understanding regarding how pain and tear size affect these kinematic patterns is minimal.
Objective: To identify relationships between pain associated with a full-thickness rotator cuff tear, tear size, and scapulohumeral rhythm (SHR) and to determine whether pain and tear size serve as predictors of SHR.
Design: A test-retest design was used to quantify pain and SHR before and after a subacromial lidocaine injection. Correlation and multivariate analyses were used to identify relationships among pain, tear size, and SHR.
Setting: Orthopaedic biomechanics research laboratory.
Patients or other participants: Fifteen patients (age range, 40-75 years) with diagnosed full-thickness rotator cuff tears participated. They were experiencing pain at the time of testing.
Intervention(s): Shoulder kinematic data were collected with an electromagnetic tracking system before and after the patient received a lidocaine injection.
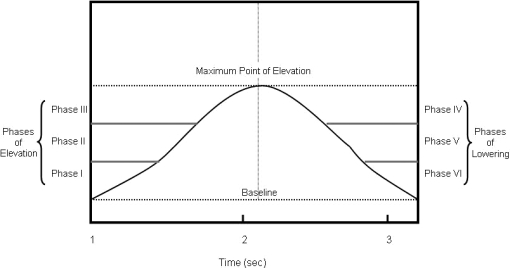
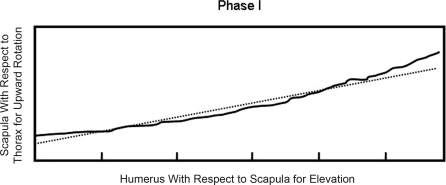
Main outcome measure(s): Pain was rated using a visual analog scale. Three-dimensional scapular kinematics and glenohumeral elevation were assessed. Scapular kinematics included anterior-posterior tilt, medial-lateral tilt, and upward-downward rotation. A regression model was used to calculate SHR (scapular kinematics to glenohumeral elevation) for phases of humeral elevation and lowering.
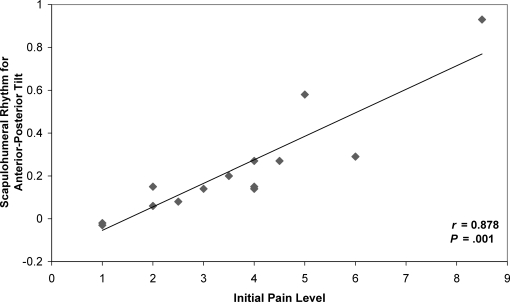
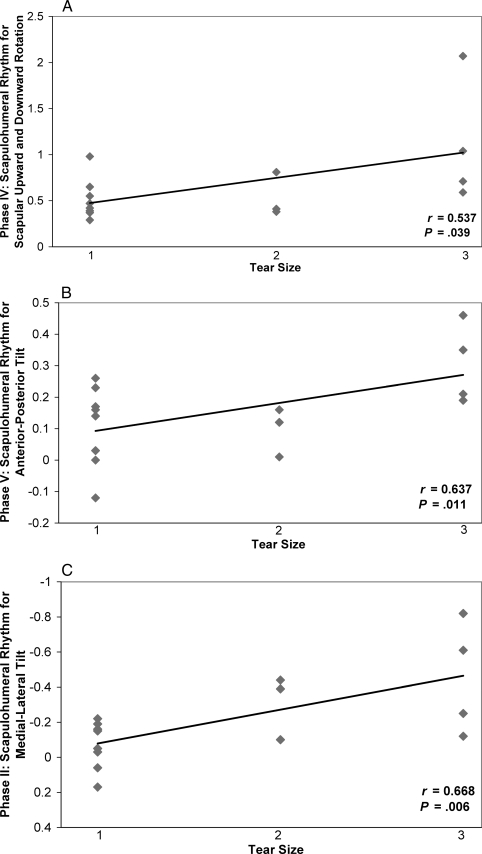
Results: Linear relationships were identified between initial pain scores and SHR and between tear size and SHR, representing an increased reliance on scapular motion with increasing pain and tear size. Pain was identified as an independent predictor of SHR, whereas significant findings for the effect of tear size on SHR and the interaction between pain and tear size were limited.
Conclusions: We noted an increased reliance on scapular contributions to overall humeral elevation with increasing levels of pain and rotator cuff tear size. Pain associated with a rotator cuff tear serves as a primary contributor to the kinematic patterns exhibited in patients with rotator cuff tears.
Keywords: biomechanics; scapula; shoulder kinematics.
Figures

Similar articles
-
Shoulder kinematics in patients with full-thickness rotator cuff tears after a subacromial injection.J Shoulder Elbow Surg. 2008 Jan-Feb;17(1):172-81. doi: 10.1016/j.jse.2007.05.010. Epub 2007 Nov 26. J Shoulder Elbow Surg. 2008. PMID: 18036839
-
How Do Scapulothoracic Kinematics During Shoulder Elevation Differ Between Adults With and Without Rotator Cuff Arthropathy?Clin Orthop Relat Res. 2020 Nov;478(11):2640-2649. doi: 10.1097/CORR.0000000000001406. Clin Orthop Relat Res. 2020. PMID: 32694316 Free PMC article.
-
Three-dimensional shoulder kinematics normalize after rotator cuff repair.J Shoulder Elbow Surg. 2016 Jun;25(6):881-9. doi: 10.1016/j.jse.2015.10.021. Epub 2016 Jan 21. J Shoulder Elbow Surg. 2016. PMID: 26803930
-
Shoulder muscle activity and function in common shoulder rehabilitation exercises.Sports Med. 2009;39(8):663-85. doi: 10.2165/00007256-200939080-00004. Sports Med. 2009. PMID: 19769415 Review.
-
Kinematic patterns in normal and degenerative shoulders. Part II: Review of 3-D scapular kinematic patterns in patients with shoulder pain, and clinical implications.Ann Phys Rehabil Med. 2018 Jan;61(1):46-53. doi: 10.1016/j.rehab.2017.09.002. Epub 2017 Oct 5. Ann Phys Rehabil Med. 2018. PMID: 28987866 Review.
Cited by
-
Return of Scapulohumeral Rhythm in Patients After Reverse Shoulder Arthroplasty: A Midterm Stereoradiographic Imaging Analysis.Iowa Orthop J. 2022 Jun;42(1):227-237. Iowa Orthop J. 2022. PMID: 35821961 Free PMC article.
-
Shoulder Coordination During Full-Can and Empty-Can Rehabilitation Exercises.J Athl Train. 2015 Nov;50(11):1117-25. doi: 10.4085/1062-6050-50.9.06. Epub 2015 Oct 9. J Athl Train. 2015. PMID: 26451620 Free PMC article.
-
Arm Position with Increased Risk of Partial Subscapularis Tear Progression Owing to Subluxation of the Long Head of Biceps Tendon: Cadaveric Biomechanical Study.Clin Orthop Surg. 2025 Aug;17(4):649-656. doi: 10.4055/cios24233. Epub 2025 Jan 10. Clin Orthop Surg. 2025. PMID: 40785757 Free PMC article.
-
Collecting shoulder kinematics with electromagnetic tracking systems and digital inclinometers: A review.World J Orthop. 2015 Nov 18;6(10):783-94. doi: 10.5312/wjo.v6.i10.783. eCollection 2015 Nov 18. World J Orthop. 2015. PMID: 26601060 Free PMC article. Review.
-
Assessment of scapulohumeral rhythm for scapular plane shoulder elevation using a modified digital inclinometer.World J Orthop. 2012 Jun 18;3(6):87-94. doi: 10.5312/wjo.v3.i6.87. World J Orthop. 2012. PMID: 22720268 Free PMC article.
References
-
- Borstad J.D, Ludewig P.M. Comparison of scapular kinematics between elevation and lowering of the arm in the scapular plane. Clin Biomech (Bristol, Avon) 2002;17(9–10):650–659. - PubMed
-
- Ludewig P.M, Cook T.M. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys Ther. 2000;80(3):276–291. - PubMed
-
- Lukasiewicz A.C, McClure P, Michener L, Pratt N, Sennett B. Comparison of 3-dimensional scapular position and orientation between subjects with and without shoulder impingement. J Orthop Sports Phys Ther. 1999;29(10):574–586. - PubMed
-
- McClure P.W, Bialker J, Neff N, Williams G, Karduna A. Shoulder function and 3-dimensional kinematics in people with shoulder impingement syndrome before and after a 6-week exercise program. Phys Ther. 2004;84(9):832–848. - PubMed
-
- Mell A.G, Hughes R.E, Carpenter J.E. Effect of rotator cuff tear size on shoulder kinematics. In: Transactions of the 51st Annual Meeting of the Orthopaedic Research Society; February 20–23, 2005; Washington, DC. Poster 0623.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
