

A clinical method for identifying scapular dyskinesis, part 2: validity
- PMID: 19295961
- PMCID: PMC2657032
- DOI: 10.4085/1062-6050-44.2.165
A clinical method for identifying scapular dyskinesis, part 2: validity
Abstract
Context: Although clinical methods for detecting scapular dyskinesis have been described, evidence supporting the validity of these methods is lacking.
Objective: To determine the validity of the scapular dyskinesis test, a visually based method of identifying abnormal scapular motion. A secondary purpose was to explore the relationship between scapular dyskinesis and shoulder symptoms.
Design: Validation study comparing 3-dimensional measures of scapular motion among participants clinically judged as having either normal motion or scapular dyskinesis.
Setting: University athletic training facilities.
Patients or other participants: A sample of 142 collegiate athletes (National Collegiate Athletic Association Division I and Division III) participating in sports requiring overhead use of the arm was rated, and 66 of these underwent 3-dimensional testing.
Intervention(s): Volunteers were viewed by 2 raters while performing weighted shoulder flexion and abduction. The right and left sides were rated independently as normal, subtle dyskinesis, or obvious dyskinesis using the scapular dyskinesis test. Symptoms were assessed using the Penn Shoulder Score.
Main outcome measure(s): Athletes judged as having either normal motion or obvious dyskinesis underwent 3-dimensional electromagnetic kinematic testing while performing the same movements. The kinematic data from both groups were compared via multifactor analysis of variance with post hoc testing using the least significant difference procedure. The relationship between symptoms and scapular dyskinesis was evaluated by odds ratios.
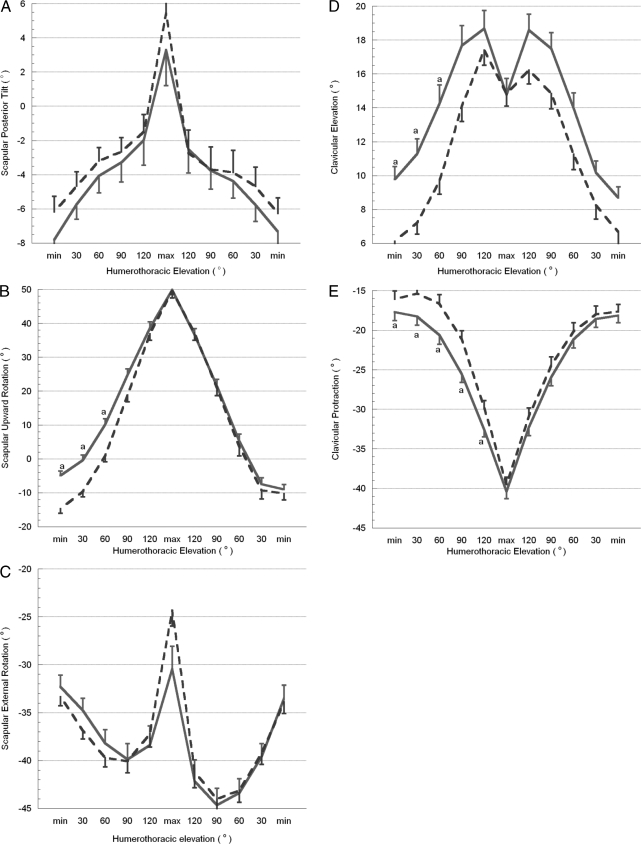
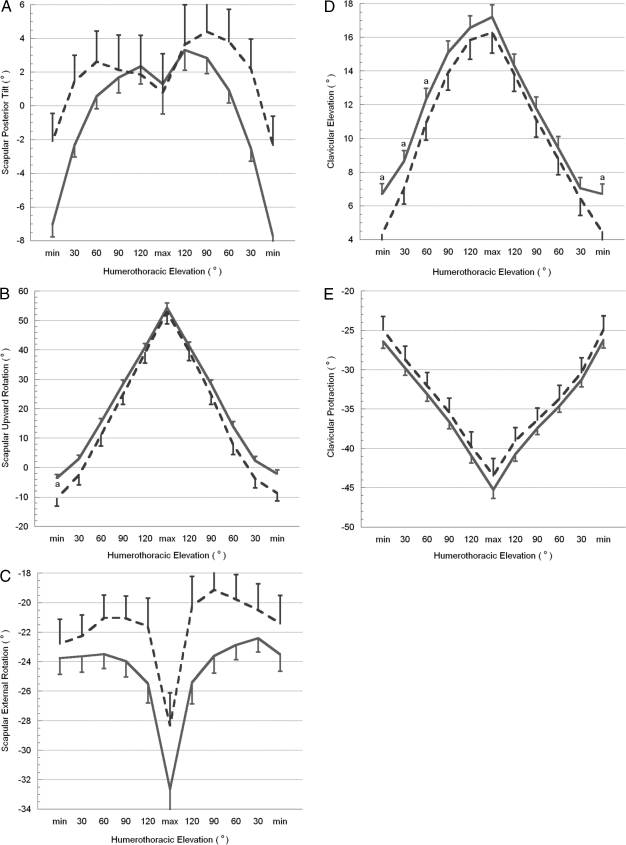
Results: Differences were found between the normal and obvious dyskinesis groups. Participants with obvious dyskinesis showed less scapular upward rotation (P < .001), less clavicular elevation (P < .001), and greater clavicular protraction (P = .044). The presence of shoulder symptoms was not different between the normal and obvious dyskinesis volunteers (odds ratio = 0.79, 95% confidence interval = 0.33, 1.89).
Conclusions: Shoulders visually judged as having dyskinesis showed distinct alterations in 3-dimensional scapular motion. However, the presence of scapular dyskinesis was not related to shoulder symptoms in athletes engaged in overhead sports.
Keywords: assessment; kinematics; shoulder; upper extremity.
Figures
Similar articles
-
A clinical method for identifying scapular dyskinesis, part 1: reliability.J Athl Train. 2009 Mar-Apr;44(2):160-4. doi: 10.4085/1062-6050-44.2.160. J Athl Train. 2009. PMID: 19295960 Free PMC article.
-
Visual scapular dyskinesis: kinematics and muscle activity alterations in patients with subacromial impingement syndrome.Arch Phys Med Rehabil. 2015 Feb;96(2):298-306. doi: 10.1016/j.apmr.2014.09.029. Epub 2014 Oct 15. Arch Phys Med Rehabil. 2015. PMID: 25449194
-
The comparison of scapular upward rotation and scapulohumeral rhythm between dominant and non-dominant shoulder in male overhead athletes and non-athletes.Man Ther. 2015 Dec;20(6):758-62. doi: 10.1016/j.math.2015.02.010. Epub 2015 Mar 5. Man Ther. 2015. PMID: 25795109
-
The shoulder joint complex in the throwing motion.J Shoulder Elbow Surg. 2024 Feb;33(2):443-449. doi: 10.1016/j.jse.2023.06.031. Epub 2023 Jul 26. J Shoulder Elbow Surg. 2024. PMID: 37499784 Review.
-
Clinical implications of scapular dyskinesis in shoulder injury: the 2013 consensus statement from the 'Scapular Summit'.Br J Sports Med. 2013 Sep;47(14):877-85. doi: 10.1136/bjsports-2013-092425. Epub 2013 Apr 11. Br J Sports Med. 2013. PMID: 23580420
Cited by
-
Reliability of scapular classification in examination of professional baseball players.Clin Orthop Relat Res. 2012 Jun;470(6):1540-4. doi: 10.1007/s11999-011-2216-0. Clin Orthop Relat Res. 2012. PMID: 22167659 Free PMC article.
-
Scapular dyskinesia: evolution towards a systems-based approach.Shoulder Elbow. 2016 Jan;8(1):61-70. doi: 10.1177/1758573215618857. Epub 2015 Dec 17. Shoulder Elbow. 2016. PMID: 27583003 Free PMC article.
-
CLINICAL RELIABILITY AND DIAGNOSTIC ACCURACY OF VISUAL SCAPULOHUMERAL MOVEMENT EVALUATION IN DETECTING PATIENTS WITH SHOULDER IMPAIRMENT.Int J Sports Phys Ther. 2015 Aug;10(4):456-63. Int J Sports Phys Ther. 2015. PMID: 26346446 Free PMC article.
-
Online supervised versus workplace corrective exercises for upper crossed syndrome: a protocol for a randomized controlled trial.Trials. 2021 Dec 11;22(1):907. doi: 10.1186/s13063-021-05875-5. Trials. 2021. PMID: 34895301 Free PMC article.
-
Validation of a new method for assessing scapular anterior-posterior tilt.Int J Sports Phys Ther. 2014 Oct;9(5):644-56. Int J Sports Phys Ther. 2014. PMID: 25328827 Free PMC article.
References
-
- Warner J.J, Micheli L.J, Arslanian L.E, Kennedy J, Kennedy R. Scapulothoracic motion in normal shoulders and shoulders with glenohumeral instability and impingement syndrome: a study using Moire topographic analysis. Clin Orthop Relat Res. 1992;285:191–199. - PubMed
-
- Kibler W.B, McMullen J. Scapular dyskinesis and its relation to shoulder pain. J Am Acad Orthop Surg. 2003;11(2):142–151. - PubMed
-
- Lukasiewicz A.C, McClure P, Michener L, Pratt N, Sennett B. Comparison of 3-dimensional scapular position and orientation between subjects with and without shoulder impingement. J Orthop Sports Phys Ther. 1999;29(10):574–586. - PubMed
-
- Ludewig P.M, Cook T.M. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys Ther. 2000;80(3):276–291. - PubMed
-
- Schmitt L, Snyder-Mackler L. Role of scapular stabilizers in etiology and treatment of impingement syndrome. J Orthop Sports Phys Ther. 1999;29(1):31–38. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
