

Meta-analysis: four-drug, three-antibiotic, non-bismuth-containing "concomitant therapy" versus triple therapy for Helicobacter pylori eradication
- PMID: 19298338
- PMCID: PMC2840655
- DOI: 10.1111/j.1523-5378.2009.00671.x
Meta-analysis: four-drug, three-antibiotic, non-bismuth-containing "concomitant therapy" versus triple therapy for Helicobacter pylori eradication
Abstract
Background: Low success rates with triple therapy for Helicobacter pylori infections have prompted search for alternatives. In one, a proton-pump inhibitor (PPI) and amoxicillin was followed by the PPI plus clarithromycin and a nitroimidazole (sequential therapy); in another, these four drugs were given concomitantly (concomitant therapy).
Aim: To compare concomitant therapy with standard triple therapy for H. pylori infection.
Methods: By searching PubMed, EMBASE, the Cochrane Central Register of Controlled Trials and abstracts of major gastrointestinal meeting, two independent reviewers systemically identified randomized controlled trials (RCT) comparing concomitant quadruple to standard triple therapies as well as studies reporting eradication rates of concomitant quadruple therapy in treatment of H. pylori. Pooled eradication rates and odds ratios (OR) with 95% confidence intervals (CI) were calculated, and univariable metaregression analysis for all extracted variables was conducted.
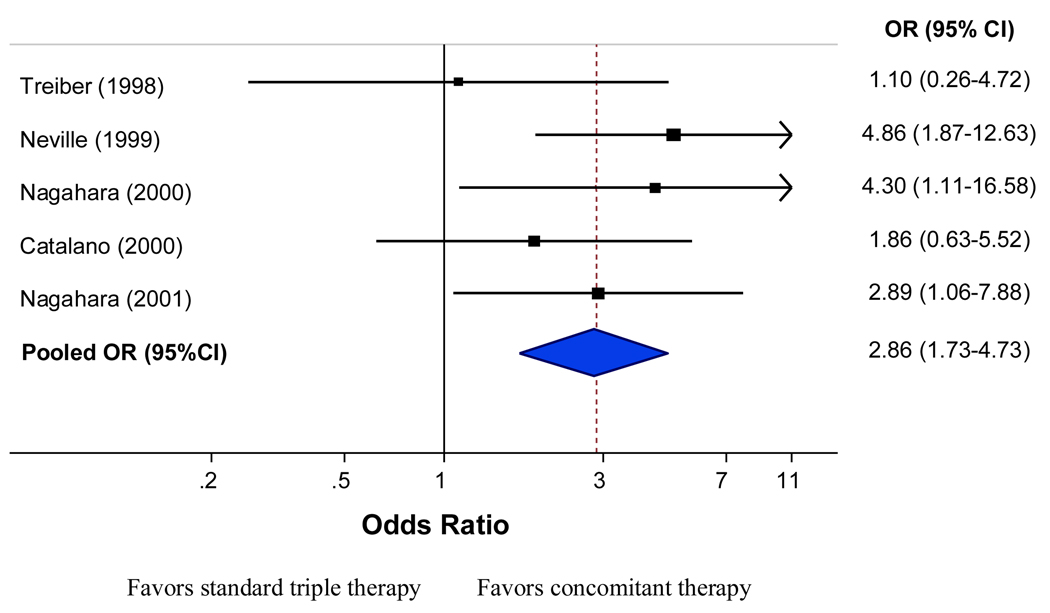
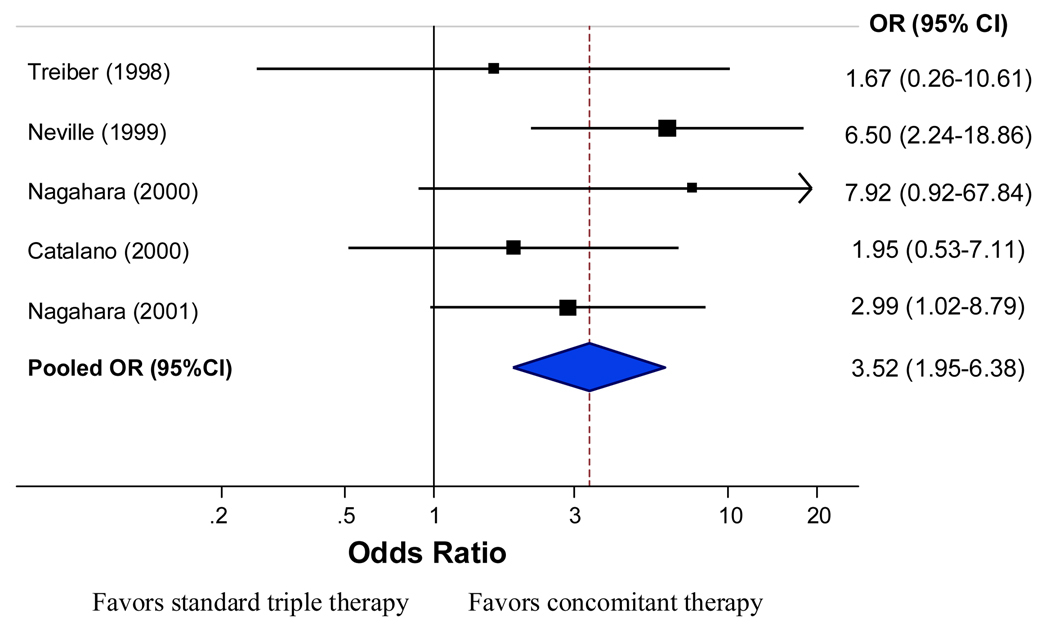
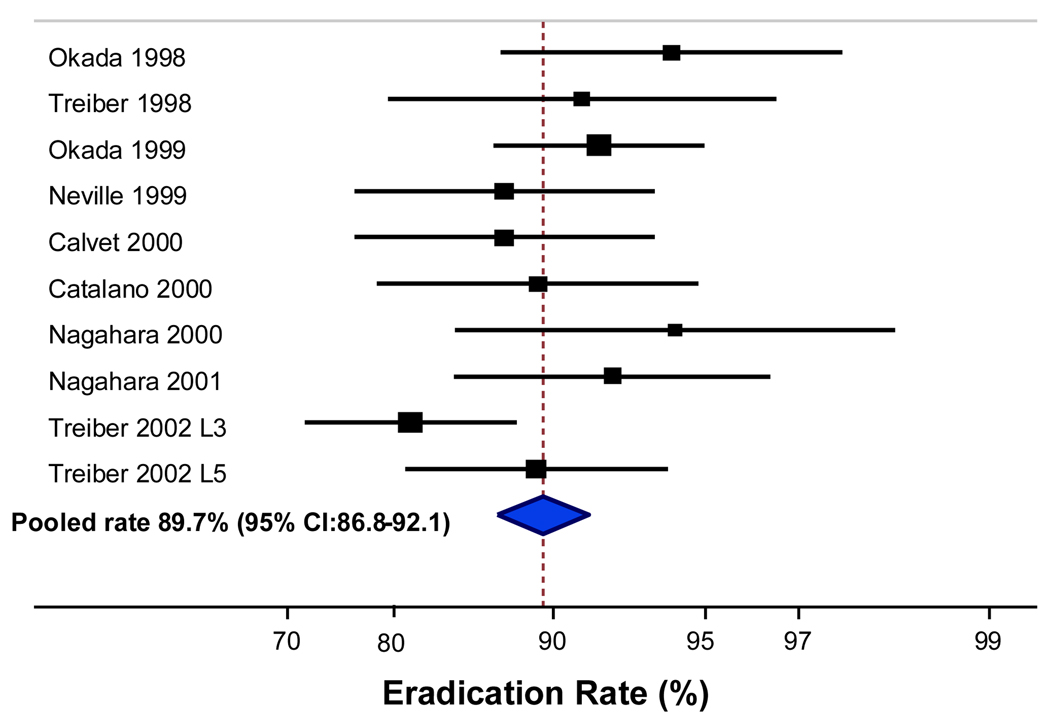
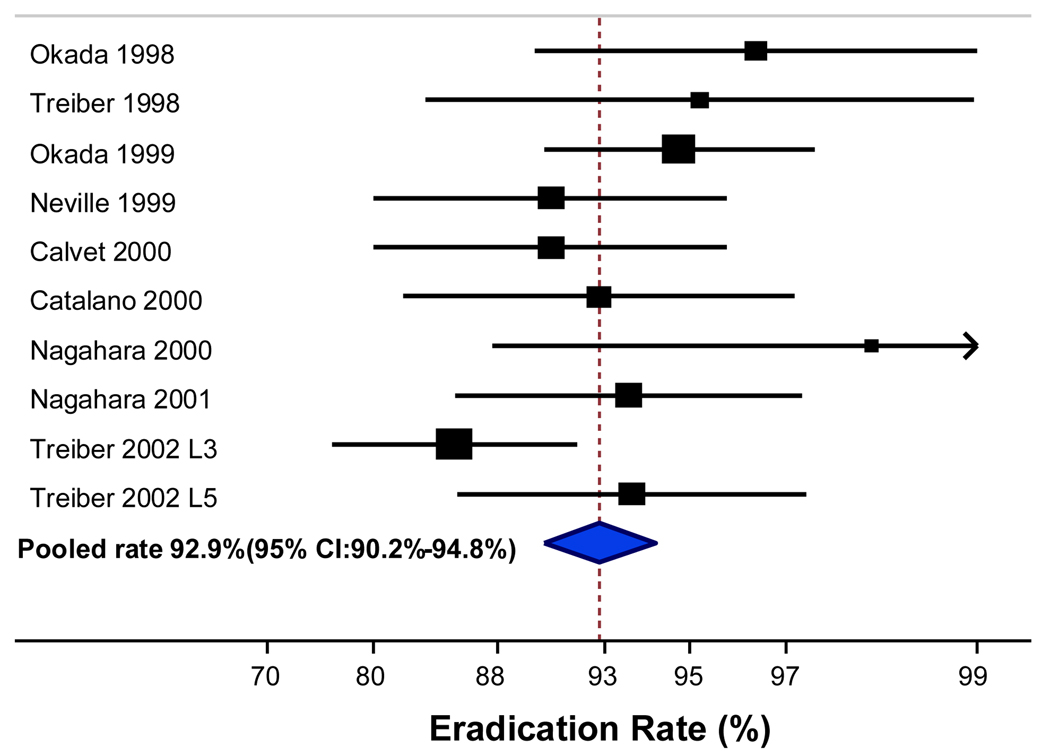
Results: We identified nine studies (10 treatment arms) including five qualifying RCTs (576 subjects) comparing concomitant (293 subjects, duration 3 to 5 days) and triple therapy (283 subjects, duration 5 to 10 days) and four other studies evaluating concomitant therapy (478 subjects, duration 3 to 7 days). Pooled estimates of the five RCTs showed superiority of concomitant therapy over triple therapy; with intention-to-treat) pooled OR of 2.86 (95% CI: 1.73-4.73) and per-protocol (PP) pooled OR of 3.52 (95% CI: 1.95-6.38). Considering all 10 treatment arms, the ITT eradication rate was 89.7% (95% CI: 86.8-92.1%) and PP was 92.9% (95% CI: 90.2-94.8%).
Conclusion: Concomitant therapy appears to be an effective alternative to triple therapy and is less complex than sequential therapy.
Figures
References
-
- Graham DY, Sung JY. Helicobacter pylori. In: Feldman M, Friedman LS, Brandt LJ, editors. Sleisenger & Fordtran's Gastrointestinal and liver disease. Pathophysiology, diagnosis, management. Philadelphia: WB Saunders Co; 2006. pp. 1049–66.
-
- Vakil N, Megraud F. Eradication therapy for Helicobacter pylori. Gastroenterology. 2007;133:985–1001. - PubMed
-
- Fischbach L, Evans EL. Meta-analysis: the effect of antibiotic resistance status on the efficacy of triple and quadruple first-line therapies for Helicobacter pylori. Aliment Pharmacol Ther. 2007;26:343–57. - PubMed
-
- Graham DY, Lu H, Yamaoka Y. A report card to grade Helicobacter pylori therapy. Helicobacter. 2007;12:275–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
