

Computerized assessment of angiographic occlusion rate and coil density in embolized human cerebral aneurysms
- PMID: 19299484
- PMCID: PMC7051637
- DOI: 10.3174/ajnr.A1463
Computerized assessment of angiographic occlusion rate and coil density in embolized human cerebral aneurysms
Abstract
Background and purpose: Computerized methods have been introduced for more objective quantification of angiographic occlusion rate and coil density as parameters of successful embolization. This study aimed 1) to evaluate this new computerized method for angiographic occlusion rating and coil density calculations by comparison with corresponding histometric parameters from retrieved human aneurysms, and 2) to compare the new computerized method with the present standard of subjective angiographic occlusion rating.
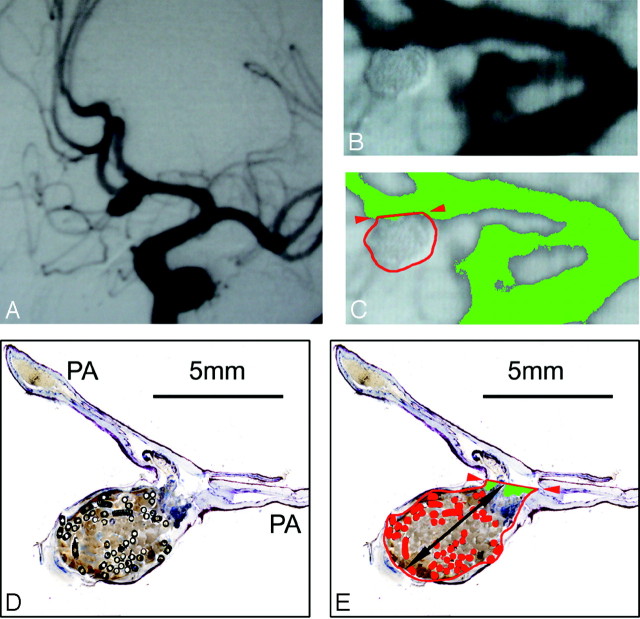
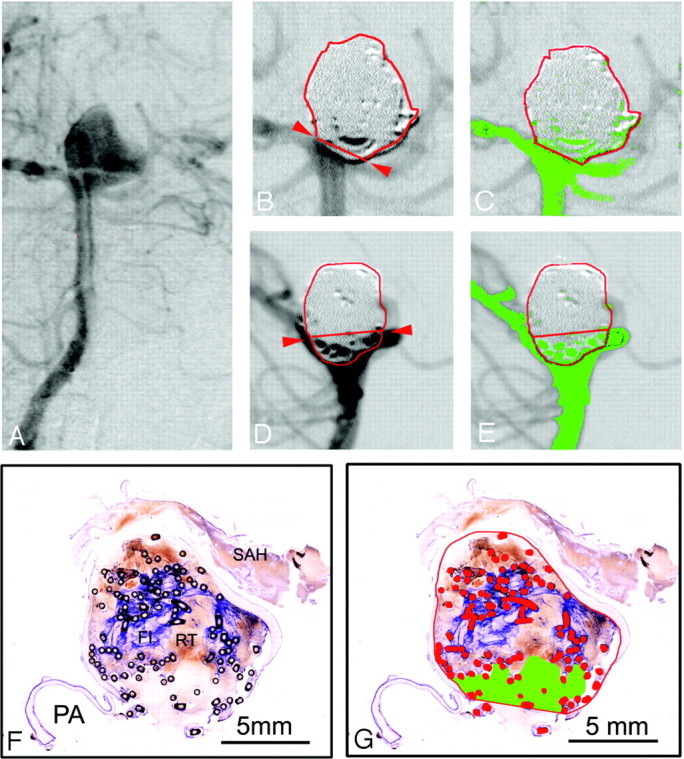
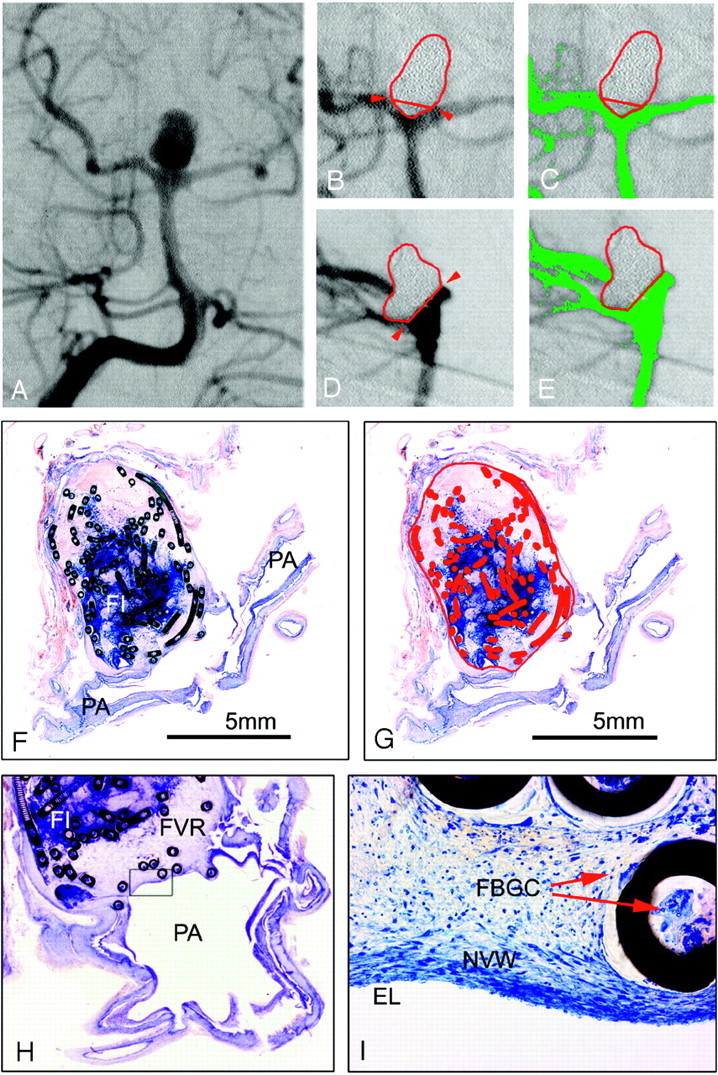
Materials and methods: From 14 postmortem-retrieved human aneurysms, angiographic occlusion rate was determined by contrast medium attenuation-gradient distinction on digital subtraction angiographs after Guglielmi detachable coil (GDC) embolization. Angiographic coil density was calculated, approximating aneurysms as ellipsoid and coils as cylindric volumes. On surface-stained histologic ground sections of the respective aneurysms, the occluded aneurysm area and coil area were measured. Then, we calculated and compared the histometric occlusion rates and coil densities with the corresponding angiographic parameters by using the Wilcoxon paired signed-rank test and the Spearman rank correlation.
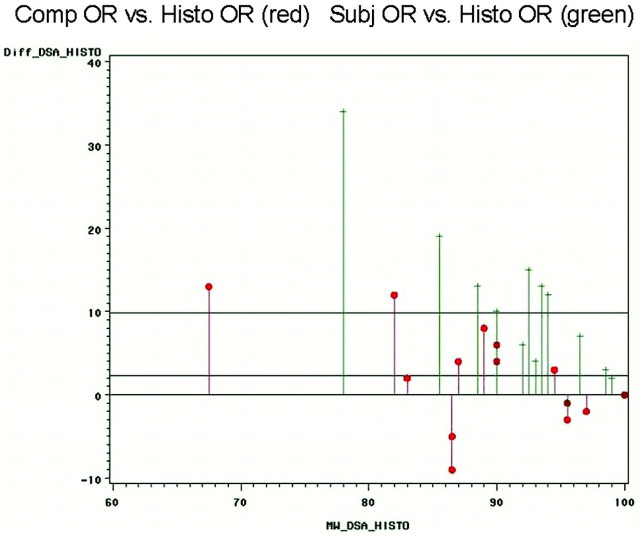
Results: Computerized angiographic occlusion rates (75%-100%) showed good correlation (r = 0.799; P < .01) with histometric occlusion-rates (61%-100%), resulting in no statistically significant differences (P = .2163). With 5.1% (+/-3.8), the mean difference between computerized angiographic occlusion rates and histometry was substantially lower compared with 10.7% (+/-8.7) mean difference between subjective angiographic estimations and histometry. Calculated angiographic coil density (13%-32%) significantly differed from histometric coil density (8%-35%; P < .05).
Conclusions: For recanalized aneurysms, computerized angiographic occlusion rating showed better correspondence with histometry compared with subjective angiographic occlusion rating. Clinical application of this new tool may lead to more objective cutoff values for re-embolization indications. The value of coil density calculations seems limited by the approximation of the aneurysms as ellipsoid volumes.
Figures
References
-
- Molyneux A, Kerr R, Stratton I, et al. International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet 2002;360:1267–74 - PubMed
-
- Molyneux A, Kerr R, Yu LM, et al. International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomized comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005;366:809–17 - PubMed
-
- Guglielmi G, Viñuela F, Sepetka I, et al. Electrothrombosis of saccular aneurysms via endovascular approach. JNS J Neurosurg 1991;75:1–7 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical