

The contribution of clinic-based interventions to reduce prenatal smoking prevalence among US women
- PMID: 19299672
- PMCID: PMC2667844
- DOI: 10.2105/AJPH.2008.144485
The contribution of clinic-based interventions to reduce prenatal smoking prevalence among US women
Abstract
Objectives: We sought to estimate the effect of universal implementation of a clinic-based, psychosocial smoking cessation intervention for pregnant women.
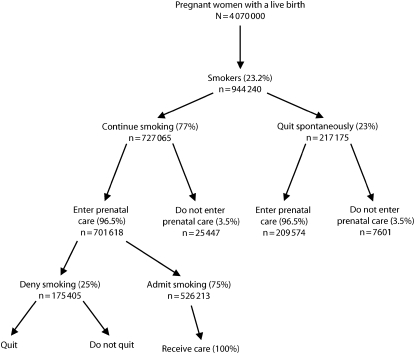
Methods: We used data from US birth certificates (2005) and the Pregnancy Risk Assessment Monitoring System (2004) to estimate the number of women smoking at conception. To calculate the number of women eligible to receive the cessation intervention, we used estimates from the literature of the percentage of women who quit spontaneously (23%), entered prenatal care before the third trimester (96.5%), and disclosed smoking to their provider (75%). We used the pooled relative risk (RR) for continued smoking from the 2004 Cochrane Review as our measure of the intervention's effectiveness (RR = 0.94).
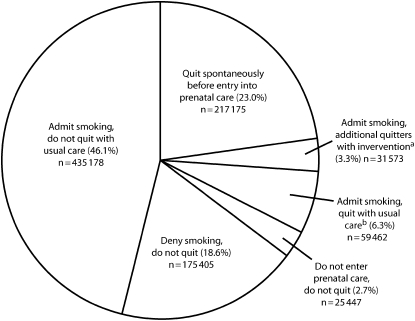
Results: We estimated that 944,240 women smoked at conception. Of these, 23.0% quit spontaneously, 6.3% quit with usual care, and an additional 3.3% quit because of the intervention, leaving 67.4% smoking throughout pregnancy. The calculated smoking prevalence in late pregnancy decreased from 16.4% to 15.6% because of the intervention.
Conclusions: Universal implementation of a best-practice, clinic-based intervention would increase the total number of quitters but would not substantially reduce smoking prevalence among pregnant women.
Figures
References
-
- Office on Smoking and Health Women and Smoking: A Report of the Surgeon General Atlanta, GA: National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention; 2001
-
- Andres RL, Day MC. Perinatal complications associated with maternal tobacco use. Semin Neonatol 2000;5:231–241 - PubMed
-
- Healthy People 2010: With Understanding and Improving Health and Objectives for Improving Health 2nd ed Washington, DC: US Dept of Health and Human Services; 2000
-
- Substance Abuse and Mental Health Services Administration Results From the 2005 National Survey on Drug Use and Health: National Findings Rockville, MD: Office of Applied Studies; 2006. NSDUH Series H-30, DHHS publication SMA 06-4194
-
- Fiore MC, Bailey WC, Cohen SJ, et al. Treating Tobacco Use and Dependence. Clinical Practice Guideline Rockville, MD: Public Health Service; 2000
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
