

Plating osteosynthesis of mid-distal humeral shaft fractures: minimally invasive versus conventional open reduction technique
- PMID: 19301000
- PMCID: PMC2899279
- DOI: 10.1007/s00264-009-0753-x
Plating osteosynthesis of mid-distal humeral shaft fractures: minimally invasive versus conventional open reduction technique
Abstract
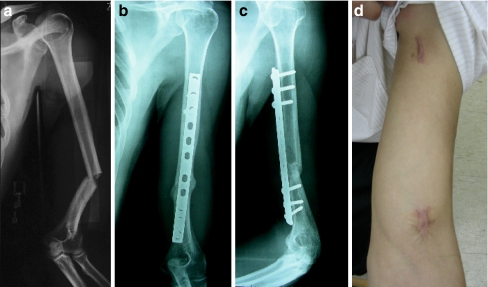
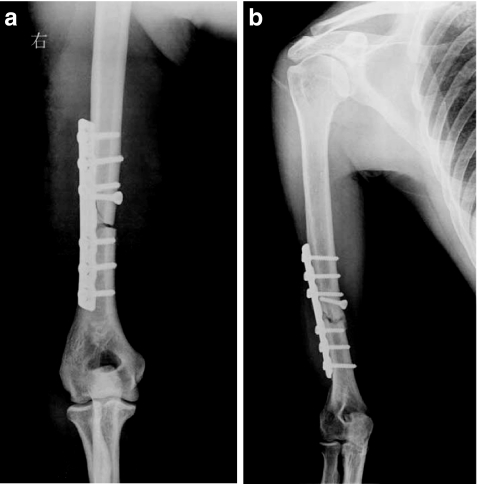
Results of two methods, conventional open reduction-internal plating and minimally invasive plating osteosynthesis (MIPO), in the treatment of mid-distal humeral shaft fractures were compared. Thirty-three patients were retrospectively analysed and divided into two groups. Group A (n = 17) patients were treated by MIPO and group B (n = 16) by conventional plating. The mean operation time in group A was 92.35 +/- 57.68 minutes and 103.12 +/- 31.08 minutes in group B (P = 0.513). Iatrogenic radial nerve palsy in group A was 0% (0/17) and 31.3% in group B (5/16 (P = 0.012). The mean fracture union time in group A was 15.29 +/- 4.01 weeks (range 8-24 weeks), and 21.25 +/- 13.67 weeks (range 10-58 weeks) in group B (P = 0.095). The mean UCLA end-result score in group A was 34.76 +/- 0.56 points (range 33-35), and 34.38 +/- 1.41 points (range 30-35) in group B (P = 0.299). The mean MEPI in group A was 99.41 +/- 2.43 points (range 90-100) and 99.69 +/- 1.25 points (range 95-100) in group B ( P = 0.687). When compared to the conventional plating techniques, MIPO offers advantages in terms of reduced incidence of iatrogenic radial nerve palsies and accelerated fracture union and a similar functional outcome with respect to shoulder and elbow function.
Les résultats de deux méthodes d’ostéosynthèse par plaques après réduction sanglante conventionnelle voie mini-invasive (MIPO) dans le traitement des fractures médio-diaphysaires de l’humérus ont été comparées. 33 patients ont été revus rétrospectivement et analysés et divisés en deux groupes : le groupe A (n = 17), traité par MIPO et le groupe B (n = 16) traité de façon conventionnelle. Le temps opératoire moyen dans le groupe A était de 92,35 +/−57,68 minutes et 103,12+/−31,08 minutes dans le groupe B (P = 0,513). Il n’a pas été observé de paralysies iatrogéniques du nerf radial dans le groupe A, par contre, dans le groupe B sont survenues 31,3% de paralysies 5/16 (p = 0,012). Le temps moyen de consolidation dans le groupe A a été de 15,29+/−4,01 semaines (8 à 24 semaines) et, dans le groupe B, de 21,25+/−13,67 semaines (10 à 58 semaines) (P = 0,095). Le score final UCLA dans le groupe A était de 34,76+/−0,56 points (33 à 35 points) et dans le groupe B de 34,38+/−1,41 points (30 à 35) (P = 0,299). Le MEPI moyen dans le groupe A a été de 99,41+/−2,43 points (de 90 à 100) et dans le groupe B de 99,69+/−1,25 points (95 à 100) (P = 0,687). Si l’on compare les deux techniques, la technique par voie mini-invasive (MIPO) permet de réduire la fréquence des paralysies du nerf radial, permet une consolidation plus rapide et une fonction similaire notamment au niveau de l’épaule et du coude.
Figures
Comment in
-
Reply to LTTE of Joshi, Anil and Singh, Saurabh: Comment on Zhiquan An et al. Plating osteosynthesis of mid-distal humeral shaft fractures: minimally invasive versus conventional open reduction technique.Int Orthop. 2010 Dec;34(8):1357. doi: 10.1007/s00264-010-1027-3. Int Orthop. 2010. PMID: 20454895 Free PMC article. No abstract available.
-
Comment on An et al.: plating osteosynthesis of mid-distal humeral shaft fractures: minimally invasive versus conventional open reduction technique.Int Orthop. 2010 Oct;34(7):1069. doi: 10.1007/s00264-010-1026-4. Epub 2010 May 11. Int Orthop. 2010. PMID: 20458479 Free PMC article. No abstract available.
References
-
- Schemitsch EH, Bhandari M (2003) Fractures of the humeral shaft. In: Browner BD, Jupiter JB, Levine AM, Trafton PG (ed) Skeletal trauma: basic science, management, and reconstruction, 3rd edn. WB Saunders Company, pp 1487–1488
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
