

Intravenous mesenchymal stem cell therapy for traumatic brain injury
- PMID: 19301973
- PMCID: PMC2889620
- DOI: 10.3171/2008.9.JNS08158
Intravenous mesenchymal stem cell therapy for traumatic brain injury
Abstract
Object: Cell therapy has shown preclinical promise in the treatment of many diseases, and its application is being translated to the clinical arena. Intravenous mesenchymal stem cell (MSC) therapy has been shown to improve functional recovery after traumatic brain injury (TBI). Herein, the authors report on their attempts to reproduce such observations, including detailed characterizations of the MSC population, non-bromodeoxyuridine-based cell labeling, macroscopic and microscopic cell tracking, quantification of cells traversing the pulmonary microvasculature, and well-validated measurement of motor and cognitive function recovery.
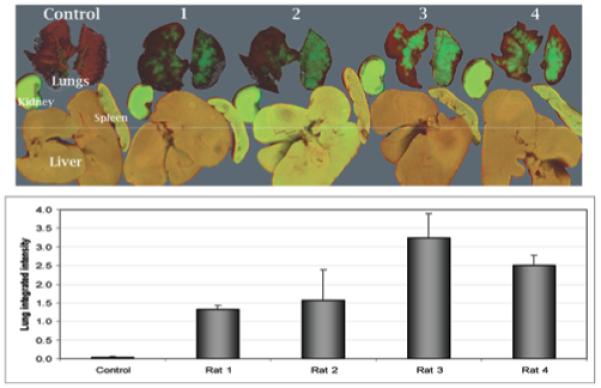
Methods: Rat MSCs were isolated, expanded in vitro, immunophenotyped, and labeled. Four million MSCs were intravenously infused into Sprague-Dawley rats 24 hours after receiving a moderate, unilateral controlled cortical impact TBI. Infrared macroscopic cell tracking was used to identify cell distribution. Immunohistochemical analysis of brain and lung tissues 48 hours and 2 weeks postinfusion revealed transplanted cells in these locations, and these cells were quantified. Intraarterial blood sampling and flow cytometry were used to quantify the number of transplanted cells reaching the arterial circulation. Motor and cognitive behavioral testing was performed to evaluate functional recovery.
Results: At 48 hours post-MSC infusion, the majority of cells were localized to the lungs. Between 1.5 and 3.7% of the infused cells were estimated to traverse the lungs and reach the arterial circulation, 0.295% reached the carotid artery, and a very small percentage reached the cerebral parenchyma (0.0005%) and remained there. Almost no cells were identified in the brain tissue at 2 weeks postinfusion. No motor or cognitive functional improvements in recovery were identified.
Conclusions: The intravenous infusion of MSCs appeared neither to result in significant acute or prolonged cerebral engraftment of cells nor to modify the recovery of motor or cognitive function. Less than 4% of the infused cells were likely to traverse the pulmonary microvasculature and reach the arterial circulation, a phenomenon termed the "pulmonary first-pass effect," which may limit the efficacy of this therapeutic approach. The data in this study contradict the findings of previous reports and highlight the potential shortcomings of acute, single-dose, intravenous MSC therapy for TBI.
Figures





References
-
- Barbash IM, Chouraqui P, Baron J, Feinberg MS, Etzion S, Tessone A, et al. Systemic delivery of bone marrow-derived mesenchymal stem cells to the infarcted myocardium: feasibility, cell migration, and body distribution. Circulation. 2003;108:863–868. - PubMed
-
- Bentzon JF, Stenderup K, Hansen FD, Schroder HD, Abdallah BM, Jensen TG, et al. Tissue distribution and engraftment of human mesenchymal stem cells immortalized by human telomerase reverse transcriptase gene. Biochem Biophys Res Commun. 2005;330:633–640. - PubMed
-
- Breyer A, Estharabadi N, Oki M, Ulloa F, Nelson-Holte M, Lien L, et al. Multipotent adult progenitor cell isolation and culture procedures. Exp Hematol. 2006;34:1596–1601. - PubMed
-
- Burns TC, Ortiz-Gonzalez XR, Gutierrez-Perez M, Keene CD, Sharda R, Demorest ZL, et al. Thymidine analogs are transferred from prelabeled donor to host cells in the central nervous system after transplantation: a word of caution. Stem Cells. 2006;24:1121–1127. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
