

Uric acid and long-term outcomes in CKD
- PMID: 19303683
- PMCID: PMC2691553
- DOI: 10.1053/j.ajkd.2008.12.021
Uric acid and long-term outcomes in CKD
Abstract
Background: Hyperuricemia is prevalent in patients with chronic kidney disease (CKD); however, data are limited about the relationship of uric acid levels with long-term outcomes in this patient population.
Study design: Cohort study.
Setting & participants: The Modification of Diet in Renal Disease (MDRD) Study was a randomized controlled trial (N = 840) conducted from 1989 to 1993 to examine the effects of strict blood pressure control and dietary protein restriction on progression of stages 3 to 4 CKD. This analysis included 838 patients.
Predictor: Uric acid level.
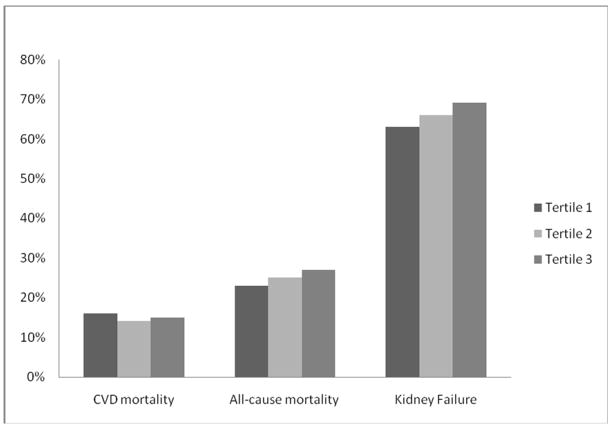
Outcomes & measurements: The study evaluated the association of baseline uric acid levels with all-cause mortality, cardiovascular disease (CVD) mortality, and kidney failure.
Results: Mean age was 52 +/- 12 (SD) years, glomerular filtration rate was 33 +/- 12 mL/min/1.73 m(2), and uric acid level was 7.63 +/- 1.66 mg/dL. During a median follow-up of 10 years, 208 (25%) participants died of any cause, 127 (15%) died of CVD, and 553 (66%) reached kidney failure. In multivariate models, the highest tertile of uric acid was associated with increased risk of all-cause mortality (hazard ratio [HR], 1.57; 95% confidence interval [CI], 1.07 to 2.32), a trend toward CVD mortality (HR, 1.47; 95% CI, 0.90 to 2.39), and no association with kidney failure (HR, 1.20; 95% CI, 0.95 to 1.51) compared with the lowest tertile. In continuous analyses, a 1-mg/dL greater uric acid level was associated with 17% increased risk of all-cause mortality (HR, 1.17; 95% CI, 1.05 to 1.30) and 16% increased risk of CVD mortality (HR, 1.16; 95% CI, 1.01 to 1.33), but was not associated with kidney failure (HR, 1.02; 95% CI, 0.97 to 1.07).
Limitations: Primary analyses were based on a single measurement of uric acid. Results are generalizable primarily to relatively young white patients with predominantly nondiabetic CKD.
Conclusions: In patients with stages 3 to 4 CKD, hyperuricemia appears to be an independent risk factor for all-cause and CVD mortality, but not kidney failure.
Figures
Comment in
-
Uric acid, cardiovascular mortality, and long-term outcomes in CKD.Am J Kidney Dis. 2009 Sep;54(3):582; author reply 582-3. doi: 10.1053/j.ajkd.2009.06.024. Am J Kidney Dis. 2009. PMID: 19700064 No abstract available.
References
-
- Bengtsson C, Lapidus L, Stendahl C, Waldenstrom J. Hyperuricaemia and risk of cardiovascular disease and overall death. A 12-year follow-up of participants in the population study of women in Gothenburg, Sweden. Acta Med Scand . 224:549–555. - PubMed
-
- Casiglia E, Spolaore P, Ginocchio G, Colangeli G, Di Menza G, Marchioro M, Mazza A, Ambrosio GB. Predictors of mortality in very old subjects aged 80 years or over. Eur J Epidemiol . 9:577–586. - PubMed
-
- Fang J, Alderman MH. Serum uric acid and cardiovascular mortality the NHANES I epidemiologic follow-up study, 1971–1992. National Health and Nutrition Examination Survey. Jama . 283:2404–2410. - PubMed
-
- Liese AD, Hense HW, Lowel H, Doring A, Tietze M, Keil U. Association of serum uric acid with all-cause and cardiovascular disease mortality and incident myocardial infarction in the MONICA Augsburg cohort. World Health Organization Monitoring Trends and Determinants in Cardiovascular Diseases. Epidemiology . 10:391–397. - PubMed
-
- Culleton BF, Larson MG, Kannel WB, Levy D. Serum uric acid and risk for cardiovascular disease and death: the Framingham Heart Study. Ann Intern Med . 131:7–13. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
