

The response of gamma vitamin E to varying dosages of alpha vitamin E plus vitamin C
- PMID: 19303966
- PMCID: PMC2688826
- DOI: 10.1016/j.metabol.2008.11.003
The response of gamma vitamin E to varying dosages of alpha vitamin E plus vitamin C
Abstract
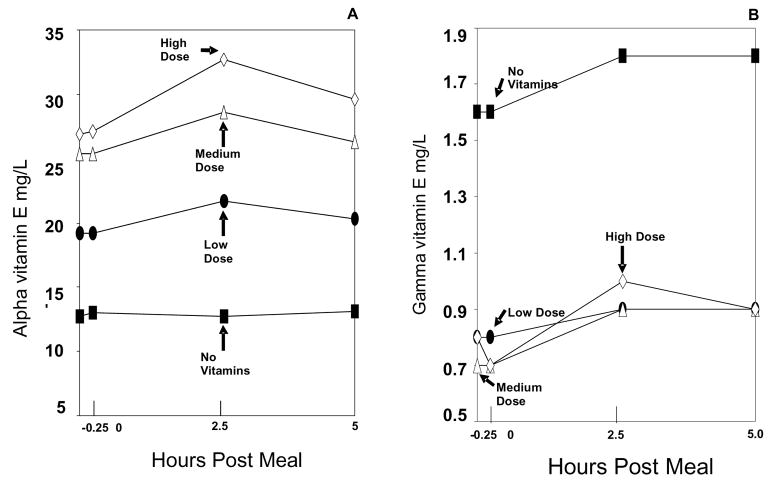
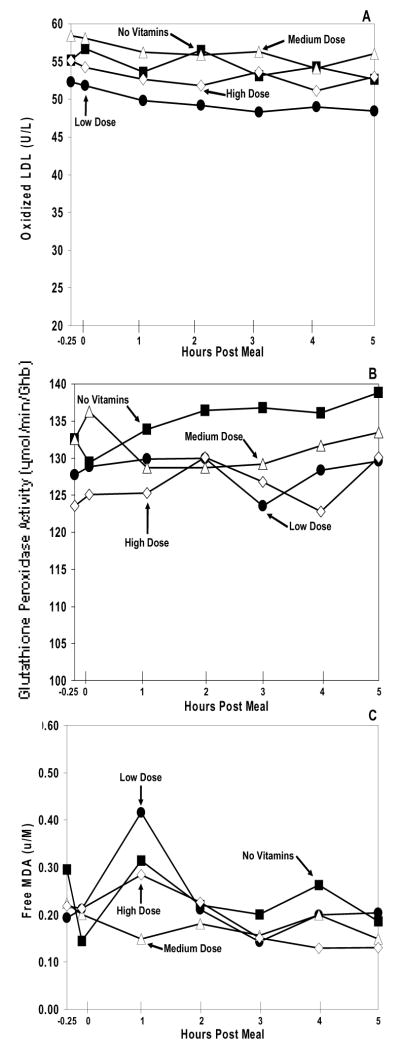
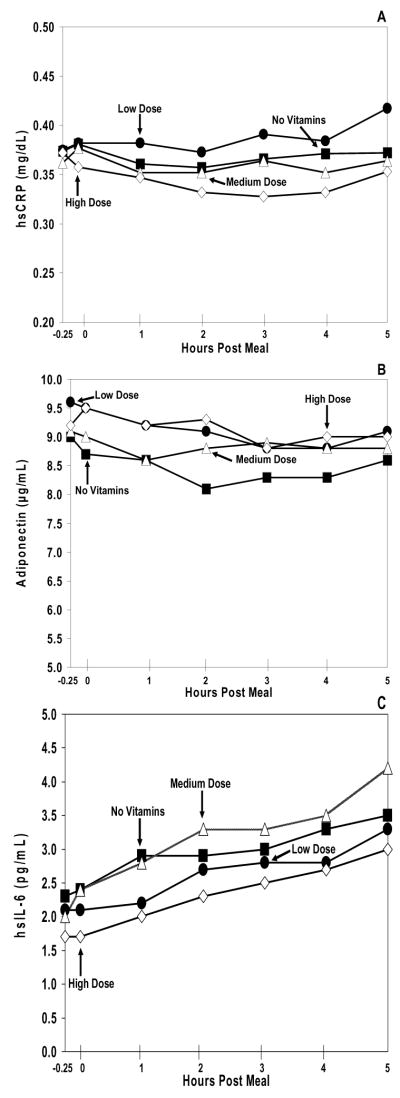
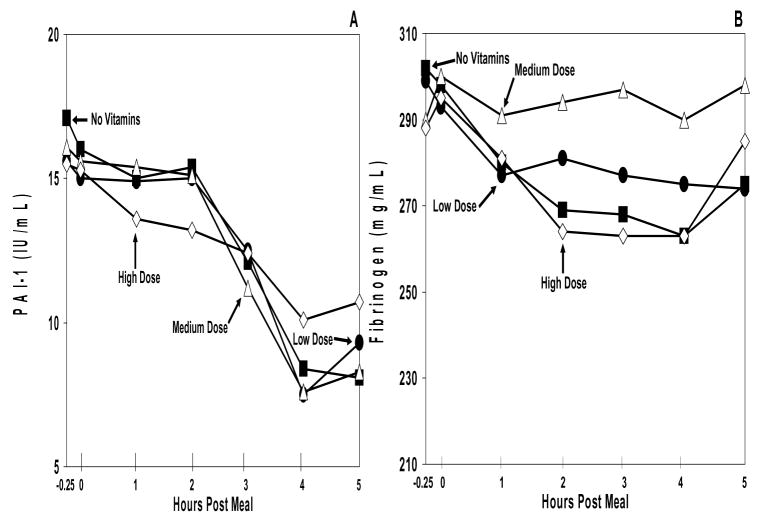
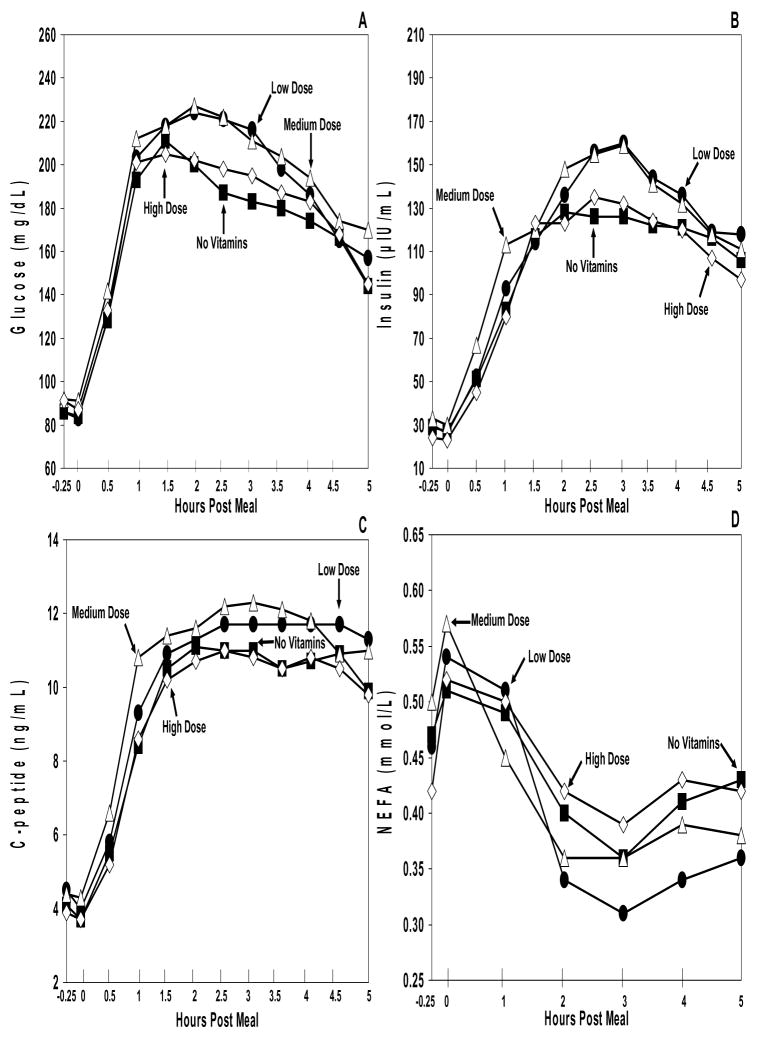
Vitamin E has been studied extensively in the prevention of atherosclerosis. Cross-sectional population studies as well as randomized controlled intervention trials have demonstrated conflicting results. A recent meta-analysis of these trials has emphasized the ineffectiveness of vitamin E in atherosclerosis prevention, with a possibility of harm at higher dosages. However, vitamin E has several isomers, with the alpha form being available via dietary supplements and the gamma form being available via dietary foodstuffs. The gamma form of vitamin E demonstrates several superior properties (such as trapping reactive nitrogen species and detoxifying nitrogen dioxide) compared with alpha vitamin E. All clinical trials have used the alpha isomer, with little concern that this isomer of vitamin E may actually suppress the gamma isomer of vitamin E. We undertook a dose-response study in volunteers with type 2 diabetes mellitus to include all the dosages of alpha vitamin E that have been used in cardiovascular prevention trials to determine the effect of alpha vitamin E on gamma vitamin E. We also assessed the effect of alpha vitamin E on several traditional markers of atherosclerotic risk. We added vitamin C to the vitamin E because several clinical trials included this vitamin to enhance the antioxidant effects of alpha vitamin E. Volunteers received, in randomized order for a 2-week period, one of the following vitamin dosage arms: (1) no vitamins, (2) low-dose supplemental vitamins E plus C, (3) medium-dose supplemental vitamins E plus C, and (4) high-dose supplemental vitamins E plus C. Blood levels of both alpha and gamma vitamin E were measured as well as surrogate markers of oxidative stress, hypercoagulation, and inflammation during a high-fat atherogenic meal (to increase the ambient oxidative stress level during the study). The results demonstrate that alpha vitamin E levels increased in proportion to the dose administered. However, at every dose of alpha vitamin E, gamma vitamin E concentration was significantly suppressed. No beneficial changes in surrogate markers of atherosclerosis were observed, consistent with the negative results of prospective clinical trials using alpha vitamin E. Our results suggest that all prospective cardiovascular clinical trials that used vitamin E supplementation actually suppressed the beneficial antioxidant gamma isomer of vitamin E. No beneficial effects on several potential cardiovascular risk factors were observed, even when the vitamin E was supplemented with vitamin C. If a standardized preparation of gamma vitamin E (without the alpha isomer) becomes available, the effects of gamma vitamin E on atherosclerotic risk will warrant additional studies.
Trial registration: ClinicalTrials.gov NCT00362518.
Figures
References
-
- Neuzil J, Weber C, Kontush A. The role of Vitamin E in atherogenesis: linking the chemical, biological and clinical aspects of the disease. Atherosclerosis. 2001;157:257–83. - PubMed
-
- Jiang Q, Christen S, Shigenaga, Ames BN. γ –Tocopherol, the major form of vitamin E in the US diet, deserves more attention. Am J Clin Nutr. 2001;74:714–22. - PubMed
-
- Rimm EB, Stampfer MJ, Ascherio A, Giovannucci E, Colditz GA, Willett WC. Vitamin E consumption and the risk of coronary heart disease in men. N Engl J Med. 1993;328(20):1450–56. - PubMed
-
- Stampfer MJ, Hennekens CH, Manson JE, Colditz GA, Willett WC. Vitamin E consumption and the risk of coronary disease in women. N Engl J Med. 1993;328(20):1444–49. - PubMed
-
- Pruthi S, Allison TG, Hensrud D. Vitamin E supplementation in the prevention of coronary heart disease. Mayo Clin Proc. 2001;76:1131–36. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
