

Mass spectrometric analysis of biomarkers and dilution markers in exhaled breath condensate reveals elevated purines in asthma and cystic fibrosis
- PMID: 19304910
- PMCID: PMC2692804
- DOI: 10.1152/ajplung.90512.2008
Mass spectrometric analysis of biomarkers and dilution markers in exhaled breath condensate reveals elevated purines in asthma and cystic fibrosis
Abstract
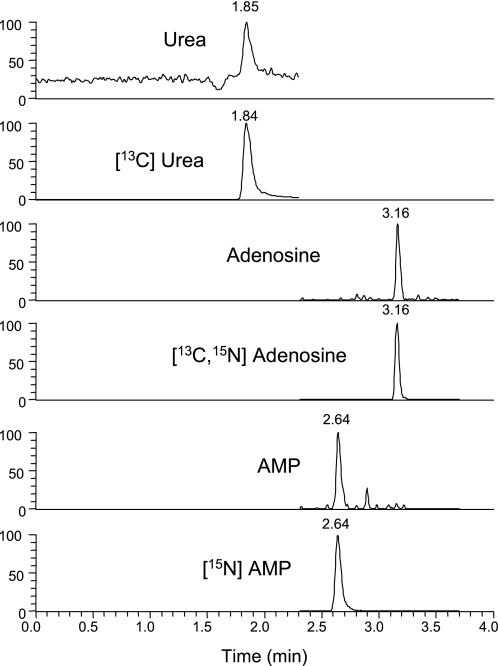
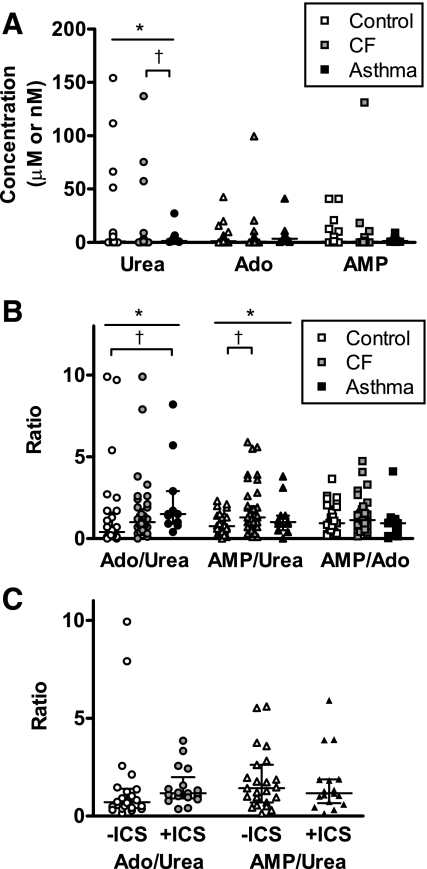
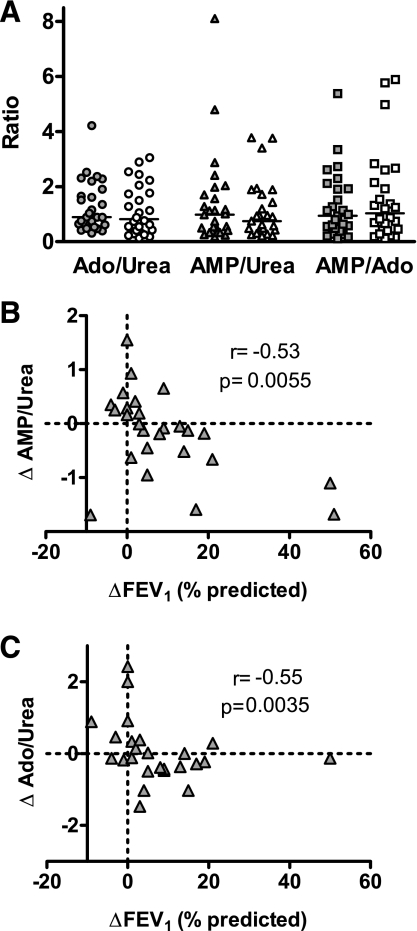
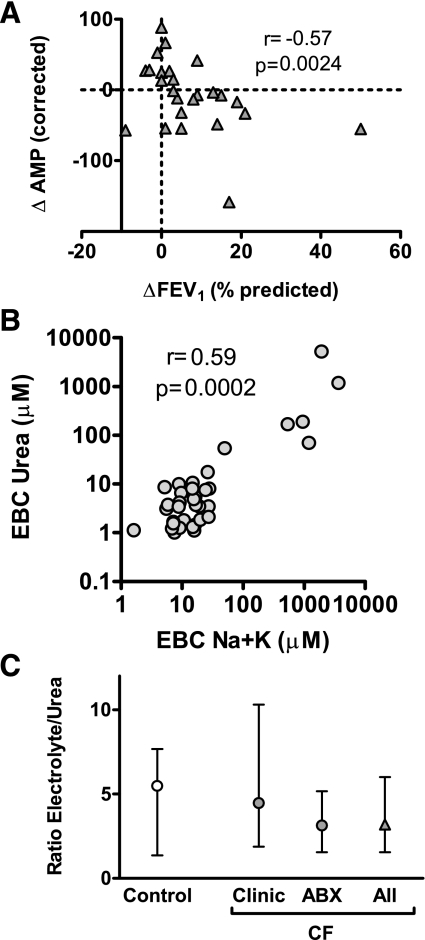
Exhaled breath condensate (EBC) analyses promise simple and noninvasive methods to measure airway biomarkers but pose considerable methodological challenges. We utilized mass spectrometry to measure EBC purine biomarkers adenosine and AMP plus urea to control for dilutional variability in two studies: 1) a cross-sectional analysis of 28 healthy, 40 cystic fibrosis (CF), and 11 asthmatic children; and 2) a longitudinal analysis of 26 CF children before and after treatment of a pulmonary exacerbation. EBC adenosine, AMP, and urea were readily detected and quantified by mass spectrometry, and analysis suggested significant dilutional variability. Using biomarker-to-urea ratios to control for dilution, the EBC AMP-to-urea ratio was elevated in CF [median 1.3, interquartile range (IQR) 0.7-2.3] vs. control (median 0.75, IQR 0.3-1.4; P < 0.05), and the adenosine-to-urea ratio was elevated in asthma (median 1.5, IQR 0.9-2.9) vs. control (median 0.4, IQR 0.2-1.6; P < 0.05). Changes in EBC purine-to-urea ratios correlated with changes in percent predicted forced expiratory volume in 1 s (FEV(1)) (r = -0.53 AMP/urea, r = -0.55 adenosine/urea; P < 0.01 for both) after CF exacerbation treatment. Similar results were observed using dilution factors calculated from serum-to-EBC urea ratios or EBC electrolytes, and the comparable ratios of EBC electrolytes to urea in CF and control (median 3.2, IQR 1.6-6.0 CF; median 5.5, IQR 1.4-7.7 control) validated use of airway urea as an EBC dilution marker. These results show that mass spectrometric analyses can be applied to measurement of purines in EBC and demonstrate that EBC adenosine-to-urea and AMP-to-urea ratios are potential noninvasive biomarkers of airways disease.
Figures
References
-
- Bloemen K, Lissens G, Desager K, Schoeters G. Determinants of variability of protein content, volume and pH of exhaled breath condensate. Respir Med 101: 1331–1337, 2007. - PubMed
-
- Bodini A, D'Orazio C, Peroni D, Corradi M, Folesani G, Baraldi E, Assael BM, Boner A, Piacentini GL. Biomarkers of neutrophilic inflammation in exhaled air of cystic fibrosis children with bacterial airway infections. Pediatr Pulmonol 40: 494–499, 2005. - PubMed
-
- Burnstock G Pathophysiology and therapeutic potential of purinergic signaling. Pharmacol Rev 58: 58–86, 2006. - PubMed
-
- Chen Y, Corriden R, Inoue Y, Yip L, Hashiguchi N, Zinkernagel A, Nizet V, Insel PA, Junger WG. ATP release guides neutrophil chemotaxis via P2Y2 and A3 receptors. Science 314: 1792–1795, 2006. - PubMed