

Income-based drug coverage in British Columbia: the impact on access to medicines
- PMID: 19305697
- PMCID: PMC2585444
Income-based drug coverage in British Columbia: the impact on access to medicines
Abstract
Background and objectives: In May 2003, the government of British Columbia adopted income-based pharmacare, replacing an age-based program. Stated policy goals included the maintenance or enhancement of access to necessary medicines. This study examines the policy impact on access to two widely used drugs for chronic risk factors (antihypertensives and statins).
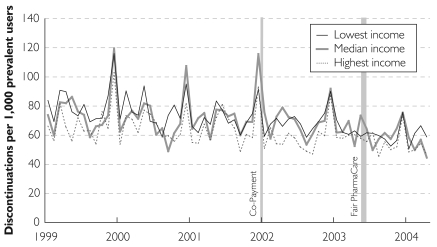
Methods: Data on incident antihypertensive and statin prescriptions between 1997 and 2004 were extracted from PharmaNet. Incident antihypertensive users were those who filled a first prescription after residing in the province for at least two years prior to the initial prescription date. The number of patients who ceased to fill a contiguous series of prescriptions (within 120 days of one another) was used as a measure of apparent discontinuation or interruption of therapy. We used time series analysis to test for changes in incident use and discontinuation.
Results: Between 1997 and 2004, 530,167 BC residents initiated therapy with an antihypertensive, and 264,904 BC residents initiated therapy with a statin. The 2003 policy change had no statistically significant impact on incident use of antihypertensives or statins, when stratified by age or income. Similarly, the 2003 policy did not change the rate of apparent discontinuations of therapy across age and income groups. However, a co-payment introduced in 2002 did increase end-of-year seasonality in apparent discontinuations in seniors--a finding that deserves further research.
Discussion: The 2003 transition to income-based pharmacare in British Columbia did not result in significant changes in access to, or continuation of, prescriptions to treat two leading chronic risk factors.
Contexte et objectifs :: En mai 2003, le gouvernement de la Colombie-Britannique a instauré un régime d’assurance-médicaments fondé sur le revenu pour remplacer un régime fondé sur l’âge. Parmi les objectifs visés, mentionnons le maintien ou l’amélioration de l’accès aux médicaments essentiels. Cette étude examine l’incidence de la politique sur l’accès à deux types de médicaments couramment utilisés pour traiter des facteurs de risque chroniques (les antihypertenseurs et les statines).
Méthodes :: On a puisé dans PharmaNet et extrait les données sur les ordonnances d’antihypertenseurs et de statines entre 1997 et 2004. Les utilisateurs ponctuels d’antihypertenseurs étaient ceux qui ont obtenu une première ordonnance après avoir résidé dans la province pendant au moins deux ans avant la date initiale de l’ordonnance. On a utilisé le nombre de patients qui ont cessé de faire exécuter une série contiguë d’ordonnances (à 120 jours d’intervalle ou moins les unes des autres) pour déterminer la cessation ou l’interruption apparente du traitement. Nous avons eu recours à l’analyse des séries chronologiques pour vérifier les changements dans l’utilisation ponctuelle et la cessation du traitement.
Résultats :: Entre 1997 et 2004, 530 167 résidents de la C.-B. ont entamé un traitement avec un antihypertenseur et 264 904 en ont entamé un avec une statine. Les changements apportés à la politique en 2003 n’ont pas eu une incidence statistiquement importante sur l’utilisation ponctuelle des antihypertenseurs ou des statines lorsqu’on les stratifie selon l’âge ou le revenu. De même, la politique de 2003 n’a pas modifié le taux de cessations apparentes du traitement pour les divers groupes d’âge ou niveaux de revenu. Cependant, une quote-part instaurée en 2002 a eu pour effet d’augmenter les fluctuations saisonnières de fin d’année dans les cessations apparentes chez les aînés – une constatation qui mérite d’être examinée de plus près.
Discussion :: L’adoption, en 2003, d’un régime d’assurance-médicaments fondé sur le revenu en Colombie-Britannique n’a pas entraîné de changements significatifs à l’accès aux médicaments ou à l’exécution ininterrompue d’ordonnances visant à traiter deux facteurs de risque chroniques.
Figures















References
-
- Hanley G.E., Morgan S., Yan L. Income-Based Drug Coverage in British Columbia: The Impact on the Distribution of Financial Burden. Healthcare Policy. 2006. http://www.longwoods.com/product.php?productid=18514&cat=458 . - PMC - PubMed
-
- Jackevicius C.A., Mamdani M., Tu J.V. Adherence with Statin Therapy in Elderly Patients with and without Acute Coronary Syndromes. Journal of the American Medical Association. 2002;288(4):462–67. - PubMed
-
- Khan N.A., McAlister F.A., Lewanczuk R.Z., Touyz R.M., Padwal R., Rabkin S.W., Leiter L.A., Lebel M., Herbert C., Schiffrin E.L., Herman R.J., Hamet P., Fodor G., Carruthers G., Culleton B., DeChamplain J., Pylypchuk G., Logan A.G., Gledhill N., Petrella R., Campbell N.R., Arnold M., Moe G., Hill M.D., Jones C., Larochelle P., Ogilvie R.I., Tobe S., Houlden R., Burgess E., Feldman R.D. The 2005 Canadian Hypertension Education Program Recommendations for the Management of Hypertension: Part II – Therapy. Canadian Journal of Cardiology. 2005;21(8):657–72. - PubMed
LinkOut - more resources
Full Text Sources