

Relationship of oxidized phospholipids on apolipoprotein B-100 particles to race/ethnicity, apolipoprotein(a) isoform size, and cardiovascular risk factors: results from the Dallas Heart Study
- PMID: 19307470
- PMCID: PMC2782388
- DOI: 10.1161/CIRCULATIONAHA.108.836940
Relationship of oxidized phospholipids on apolipoprotein B-100 particles to race/ethnicity, apolipoprotein(a) isoform size, and cardiovascular risk factors: results from the Dallas Heart Study
Abstract
Background: Elevated levels of oxidized phospholipids (OxPLs) on apolipoprotein B-100 particles (OxPL/apoB) are associated with cardiovascular disease and predict new cardiovascular events. Elevated lipoprotein (a) [Lp(a)] levels are a risk factor for cardiovascular disease in whites and also in blacks if they carry small apolipoprotein(a) [apo(a)] isoforms. The relationship of OxPL/apoB levels to race/ethnicity, cardiovascular risk factors, and apo(a) isoforms is not established.
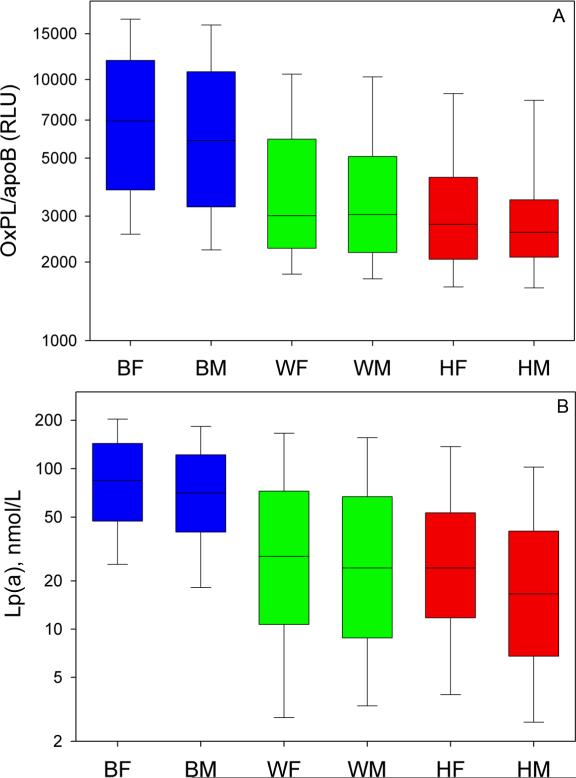
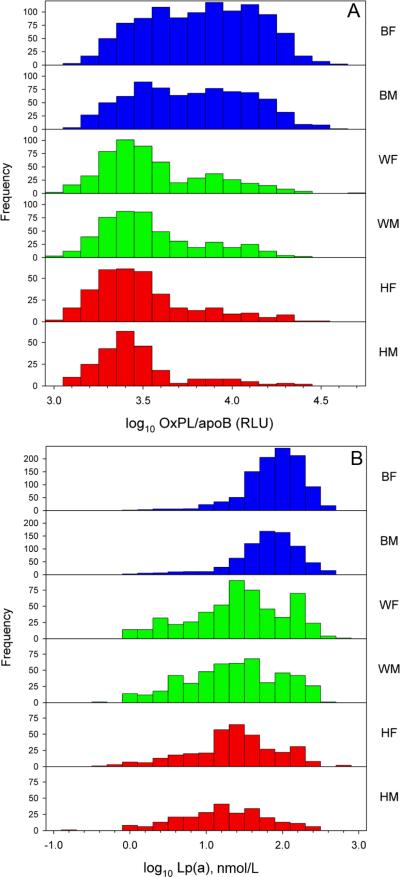
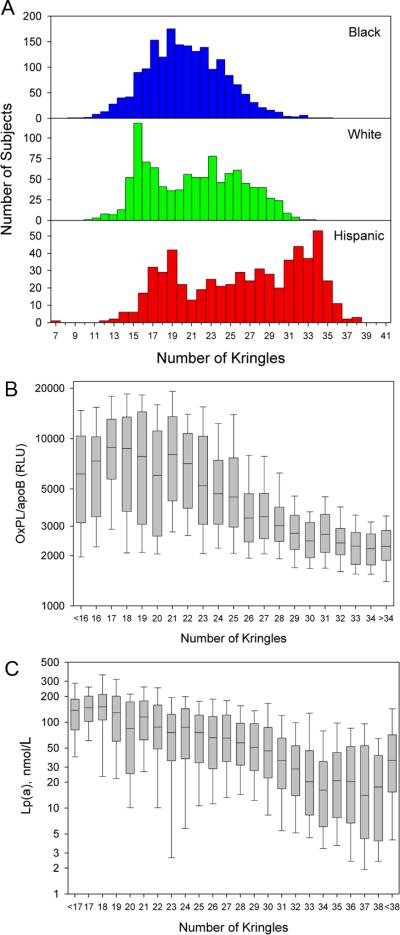
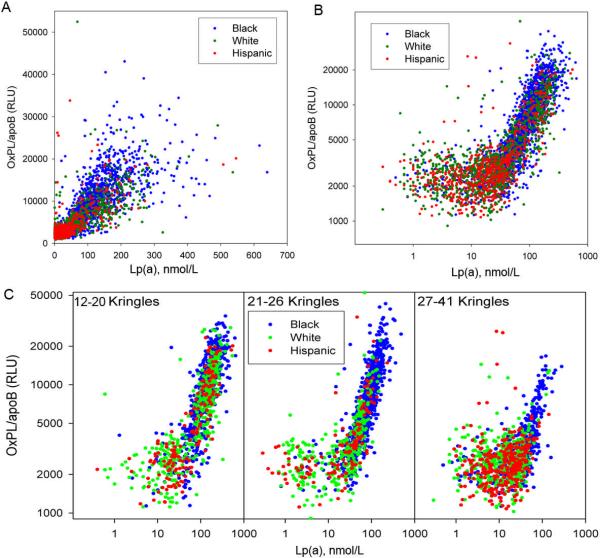
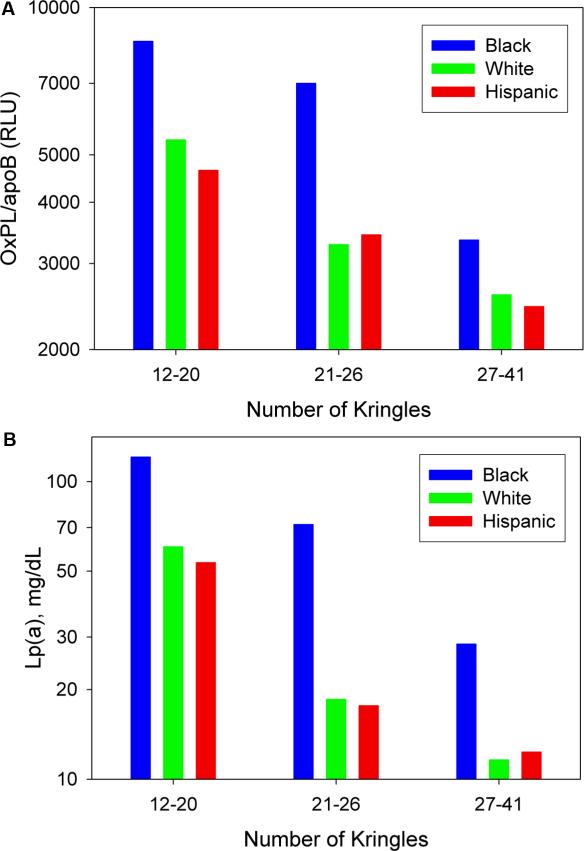
Methods and results: OxPL/apoB levels were measured in 3481 subjects (1831 black, 1047 white, and 603 Hispanic subjects) in the Dallas Heart Study and correlated with age, sex, cardiovascular risk factors, and Lp(a) and apo(a) isoforms. Significant differences in OxPL/apoB levels were noted among racial/ethnic subgroups, with blacks having the highest levels compared with whites and Hispanics (P<0.001 for each comparison). OxPL/apoB levels generally did not correlate with age, sex, or risk factors. In the overall cohort, OxPL/apoB levels strongly correlated with Lp(a) (r=0.85, P<0.001), with the shape of the relationship demonstrating a "reverse L" shape for log-transformed values. The highest correlation was present in blacks, followed by whites and Hispanics; was dependent on apo(a) isoform size; and became progressively weaker with larger isoforms. The size of the major apo(a) isoform (number of kringle type IV repeats) was negatively associated with OxPL/apoB (r=-0.49, P<0.001) and Lp(a) (r=-0.61, P<0.001) regardless of racial/ethnic group. After adjustment for apo(a) isoform size, the relationship between OxPL/apoB and Lp(a) remained significant (r=0.67, P<0.001).
Conclusions: OxPL/apoB levels vary according to race/ethnicity, are largely independent of cardiovascular risk factors, and are inversely associated with apo(a) isoform size. The association of OxPL with small apo(a) isoforms, in which a similar relationship is present among all racial/ethnic subgroups despite differences in Lp(a) levels, may be a key determinant of cardiovascular risk.
Figures
References
-
- Navab M, Ananthramaiah GM, Reddy ST, Van Lenten BJ, Ansell BJ, Fonarow GC, Vahabzadeh K, Hama S, Hough G, Kamranpour N, Berliner JA, Lusis AJ, Fogelman AM. Thematic review series: The Pathogenesis of atherosclerosis: The oxidation hypothesis of atherogenesis: the role of oxidized phospholipids and HDL. J Lipid Res. 2004;45:993–1007. - PubMed
-
- Tsimikas S, Brilakis ES, Miller ER, McConnell JP, Lennon RJ, Kornman KS, Witztum JL, Berger PB. Oxidized phospholipids, Lp(a) lipoprotein, and coronary artery disease. N Engl J Med. 2005;353:46–57. - PubMed
-
- Tsimikas S, Kiechl S, Willeit J, Mayr M, Miller ER, Kronenberg F, Xu Q, Bergmark C, Weger S, Oberhollenzer F, Witztum JL. Oxidized phospholipids predict the presence and progression of carotid and femoral atherosclerosis and symptomatic cardiovascular disease: five-year prospective results from the Bruneck study. J Am Coll Cardiol. 2006;47:2219–2228. - PubMed
-
- Tsimikas S, Bergmark C, Beyer RW, Patel R, Pattison J, Miller E, Juliano J, Witztum JL. Temporal increases in plasma markers of oxidized low-density lipoprotein strongly reflect the presence of acute coronary syndromes. J Am Coll Cardiol. 2003;41:360–370. - PubMed
-
- Tsimikas S, Lau HK, Han KR, Shortal B, Miller ER, Segev A, Curtiss LK, Witztum JL, Strauss BH. Percutaneous coronary intervention results in acute increases in oxidized phospholipids and lipoprotein(a): Short-term and long-term immunologic responses to oxidized low-density lipoprotein. Circulation. 2004;109:3164–3170. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
