

Phase II studies of gemcitabine and cisplatin in heavily and minimally pretreated metastatic breast cancer
- PMID: 19307510
- PMCID: PMC2674003
- DOI: 10.1200/JCO.2008.17.4839
Phase II studies of gemcitabine and cisplatin in heavily and minimally pretreated metastatic breast cancer
Abstract
Purpose: Cisplatin and gemcitabine have single-agent activity in metastatic breast cancer, and preclinical data support synergy of the combination. Two parallel, phase II trials were conducted to evaluate the response rate, response duration, and toxicities of the combination. Genetic polymorphisms were analyzed for correlation with outcomes.
Patients and methods: Eligible women had measurable disease and heavily or minimally pretreated metastatic breast cancer. The heavily pretreated protocol required prior anthracycline and taxane therapy; cisplatin as part of high-dose therapy was allowed. All patients received cisplatin 25 mg/m(2) on days 1 through 4 and gemcitabine 1,000 mg/m(2) on days 2 and 8 of a 21-day cycle with prophylactic granulocyte colony-stimulating factor in the heavily pretreated group. Sera from a subset of patients were evaluated by polymerase chain reaction restriction fragment length polymorphism for polymorphisms in 10 genes of interest.
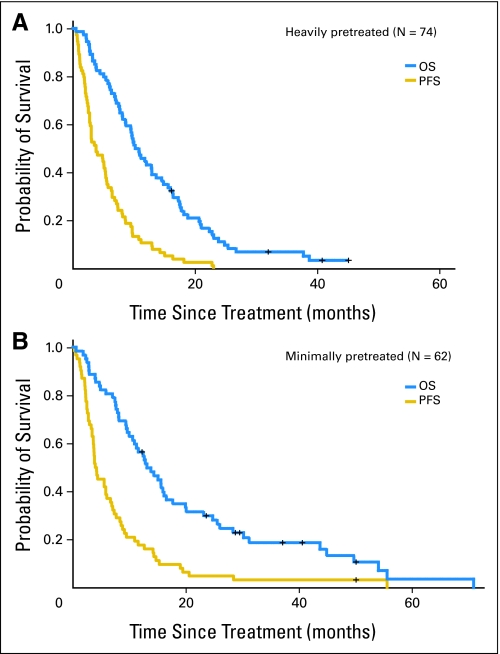
Results: Of 136 women enrolled, 74 were heavily pretreated. Both protocols accrued to their two-stage design. The response rate for both the heavily and minimally pretreated cohorts was 26%, and the median durations of response were 5.3 and 5.9 months, respectively. In a multivariate analysis, hormone receptor-negative disease was associated with a higher response rate. The most common grades 3 or 4 toxicities were thrombocytopenia (71%), neutropenia (66%), and anemia (38%). In a subset of 55 patients, the xeroderma pigmentosum group D (XPD)-751, x-ray cross-complementing group 3 (XRCC3) and cytidine deaminase polymorphisms were significantly associated with clinical outcomes.
Conclusion: Combination cisplatin and gemcitabine is active in metastatic breast cancer regardless of prior therapy. Genetic polymorphisms may tailor which patients benefit from this regimen.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Henderson IC, Berry DA, Demetri GD, et al. Improved outcomes from adding sequential paclitaxel but not from escalating doxorubicin dose in an adjuvant chemotherapy regimen for patients with node-positive primary breast cancer. J Clin Oncol. 2003;21:976–983. - PubMed
-
- Mamounas EP, Bryant J, Lembersky B, et al. Paclitaxel after doxorubicin plus cyclophosphamide as adjuvant chemotherapy for node-positive breast cancer: Results from NSABP B-28. J Clin Oncol. 2005;23:3686–3696. - PubMed
-
- Martin M, Pienkowski T, Mackey J, et al. Adjuvant docetaxel for node-positive breast cancer. N Engl J Med. 2005;352:2302–2313. - PubMed
-
- Sledge GW, Jr, Loehrer PJ, Sr, Roth BJ, et al. Cisplatin as first-line therapy for metastatic breast cancer. J Clin Oncol. 1988;6:1811–1814. - PubMed
-
- Carmichael J, Possinger K, Phillip P, et al. Advanced breast cancer: A phase II trial with gemcitabine. J Clin Oncol. 1995;13:2731–2736. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
