

Free vascularised fibular grafting in the treatment of large skeletal defects due to osteomyelitis
- PMID: 19308407
- PMCID: PMC2899305
- DOI: 10.1007/s00264-009-0761-x
Free vascularised fibular grafting in the treatment of large skeletal defects due to osteomyelitis
Abstract
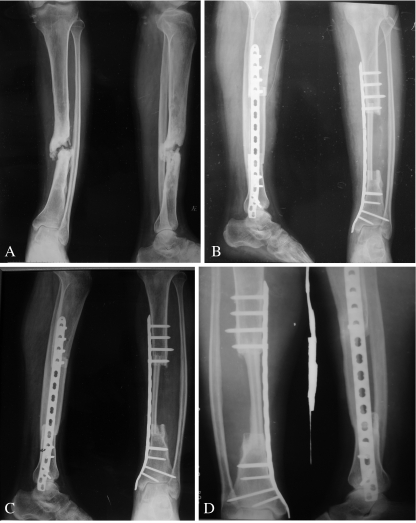
Treatment of skeletal defects secondary to osteomyelitis is a challenging problem. The purpose of this study was to present our experience of the use of free vascularised fibular grafts to treat such defects. Ten patients with a mean age of 31 years (range 16-50 years) and a skeletal defect with a mean length of 9.5 cm (range 6-17 cm) were managed with a protocol which included radical debridement of the lesion and a vascularised fibular graft. The mean follow-up time was 26 months. Union of the graft occurred in all patients, at a mean of 4.5 months. No recurrence of osteomyelitis was observed. The mean time to full weight bearing was ten months, and all patients were pain-free and able to walk without supportive devices. A free vascularised fibular graft is a viable option for the management of large skeletal defects resulting from osteomyelitis.
Figures

References
-
- Cattaneo R, Catagni MA, Johnson EE. The treatment of infected nonunion and segmental defects of the tibia by the methods of Ilizarov. Clin Orthop Relat Res. 1992;280:143–152. - PubMed
-
- Dormans JP, Krajbich JI, Zuker R, et al. Congenital pseudarthrosis of the tibia: treatment with free vascularized fibular grafts. J Pediatr Orthop. 1990;10:623–628. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
