

Current approach to fibrous dysplasia of bone and McCune-Albright syndrome
- PMID: 19308500
- PMCID: PMC2656698
- DOI: 10.1007/s11832-007-0006-8
Current approach to fibrous dysplasia of bone and McCune-Albright syndrome
Abstract
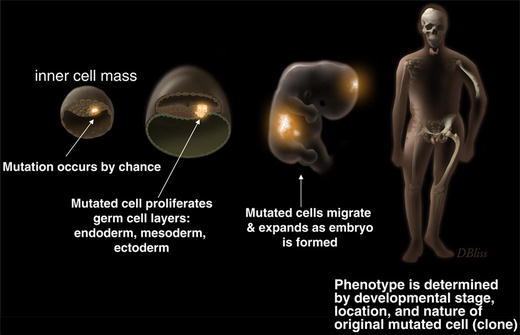
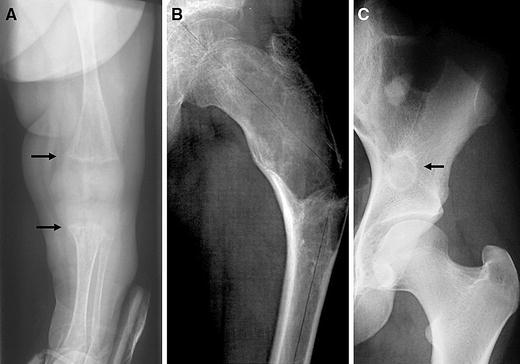
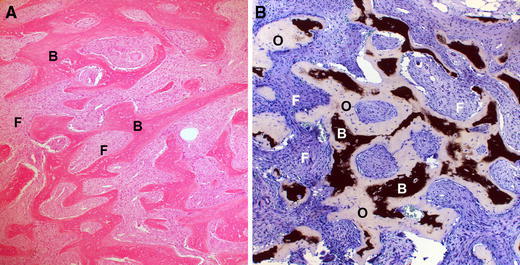
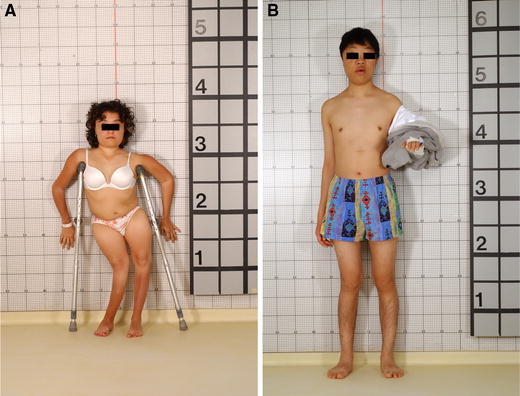
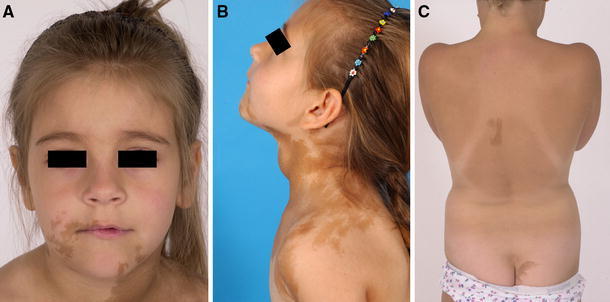
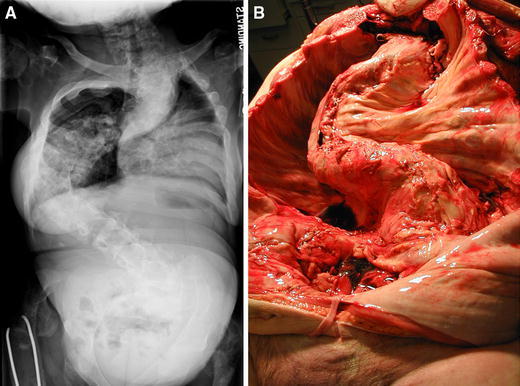
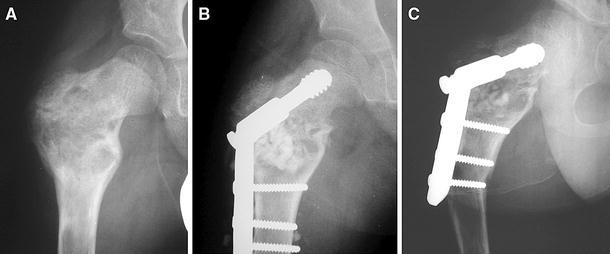
Fibrous dysplasia (FD) of bone is an uncommon disease caused by sporadic, congenital mutations in the cAMP regulating protein, G(s)alpha. It is an example of somatic mosaicism in which a wide spectrum of disease is possible. Widespread skeletal involvement is often associated with varying combinations of café-au-lait skin spots, and/or endocrine dysfunction (precocious puberty, renal phosphate wasting, hyperthyroidism, and/or growth hormone excess). Unrecognized and untreated endocrine dysfunction can exacerbate the skeletal disease. The diagnosis is usually established on clinical grounds on the basis of physical examination and typical radiographic appearance. Occasionally, gene testing of affected tissue may be helpful. The skeletal sites involved with disease are established at an early age, and the complications of fracture deformity are most pronounced in childhood. Bone pain in the absence of a fracture is more common in adults, but can also be present in children. Treatment with bisphosphonates is usually effective at relieving pain, but probably has no effect on the natural history of the disease. Scoliosis, which was previously thought to be an uncommon occurrence, has been shown to be common and progressive, and as such, warrants investigation and, when necessary, surgical treatment. The surgical management of FD remains challenging. Timing and technique remain controversial, but some consensus exists in that grafting materials (of any type) usually fail and should not be a central aspect of the surgical approach. Intramedullary devices are in general superior to side plates and screws. In extremely widespread disease with very early fracture and deformity, no surgical approach will affect final functional outcome. Efforts should be made for the initiation of international collaborative studies to better define optimal surgical approaches to the treatment of this challenging disease.
Figures



References
-
- McCune DJ. Osteitis fibrosa cystica: the case of a nine-year-old girl who also exhibits precocious puberty, multiple pigmentation of the skin and hyperthyroidism. Am J Dis Child. 1936;52:743–744.
-
- Albright F, Butler AM, Hampton AO, Smith P. Syndrome characterized by osteitis fibrosa disseminata, areas, of pigmentation, and endocrine dysfunction, with precocious puberty in females: report of 5 cases. N Engl J Med. 1937;216:727–746. doi: 10.1056/NEJM193704292161701. - DOI
-
- Lichtenstein L. Polyostotic fibrous dysplasia. Arch Surg. 1938;36:874–898. doi: 10.1001/archsurg.1938.01190230153012. - DOI
-
- Lichtenstein L, Jaffe HL. Fibrous dysplasia of bone: a condition affecting one, several or many bones, graver cases of which may present abnormal pigmentation of skin, premature sexual development, hyperthyroidism or still other extraskeletal abnormalities. Arch Pathol. 1942;33:777–816.
-
- Dorfman HD, Czerniak B (1998) Fibroosseous lesions. In: Dorfman HD, Czerniak B (eds) Bone tumors. Mosby, St. Louis, pp 441–491
LinkOut - more resources
Full Text Sources
