

Lower-limb growth: how predictable are predictions?
- PMID: 19308536
- PMCID: PMC2656868
- DOI: 10.1007/s11832-008-0119-8
Lower-limb growth: how predictable are predictions?
Abstract
Purpose: The purpose of this review is to clarify the different methods of predictions for growth of the lower limb and to propose a simplified method to calculate the final limb deficit and the correct timing of epiphysiodesis.
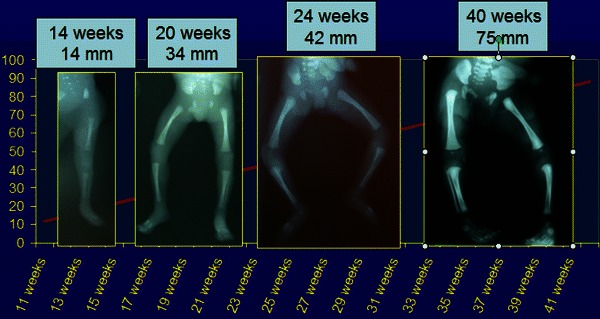
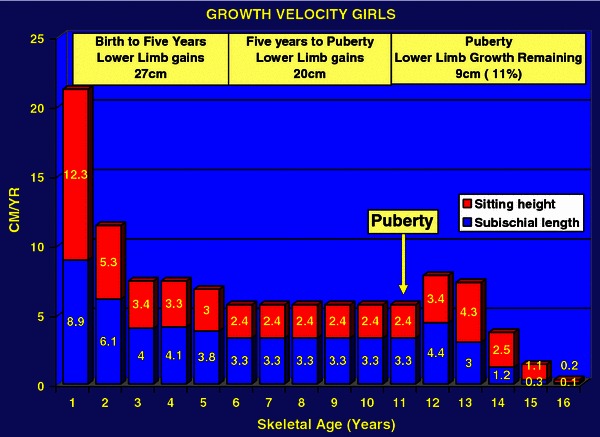
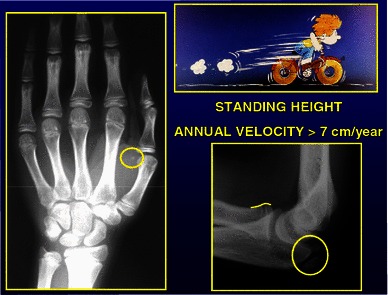
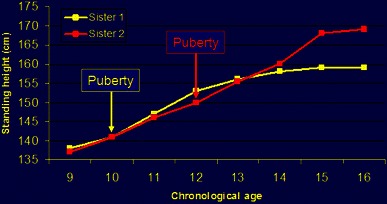
Background: Lower-limb growth is characterized by four different periods: antenatal growth (exponential); birth to 5 years (rapid growth); 5 years to puberty (stable growth); and puberty, which is the final growth spurt characterized by a rapid acceleration phase lasting 1 year followed by a more gradual deceleration phase lasting 1.5 years. The younger the child, the less precise is the prediction. Repeating measurements can increase the accuracy of predictions and those calculated at the beginning of puberty are the most accurate. The challenge is to reduce the margin of uncertainty. Confrontation of the different parameters-bone age, Tanner signs, annual growth velocity of the standing height, sub-ischial length and sitting height-is the most accurate method. Charts and diagrams are only models and templates. There are many mathematical equations in the literature; we must be able to step back from these rigid calculations because they are a false guarantee. The dynamic of growth needs a flexible approach. There are, however, some rules of thumb that may be helpful for different clinical scenarios.
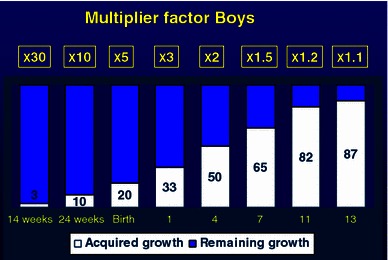
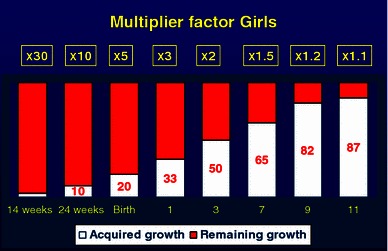
Calculation of limb length discrepancy: For congenital malformations, at birth the limb length discrepancy must be multiplied by 5 to give the final limb length discrepancy. Multiple by 3 at 1 year of age; by 2 at 3 years in girls and 4 years in boys; by 1.5 at 7 years in girls and boys, by 1.2 at 9 years in girls and 11 years in boys and by 1.1 at the onset of puberty (11 years bone age for girls and 13 years bone age for boys).
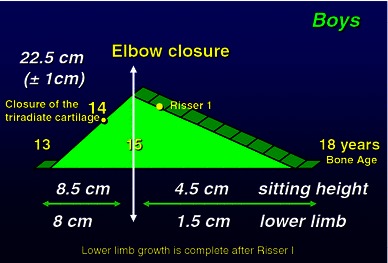
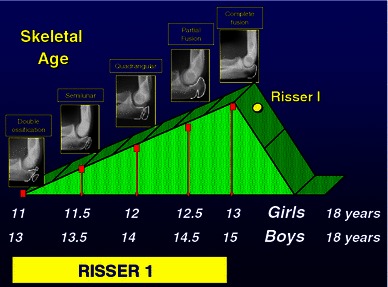
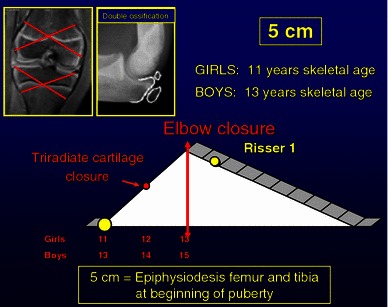
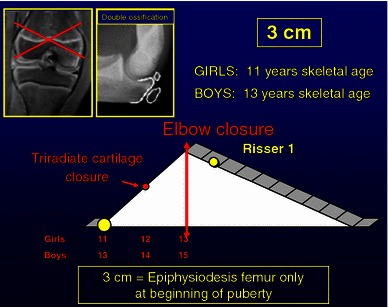
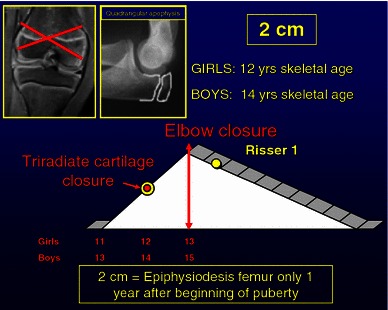
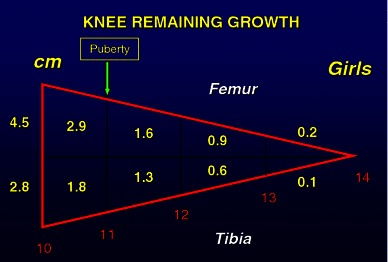
Timing of epiphysiodesis: For the timing of epiphysiodesis, several simple principles must be observed to reduce the margin of error; strict and repeated measurements, rigorous analysis of the data obtained, perfect evaluation of bone age with elbow plus hand radiographs and confirmation with Tanner signs. The decision should always be taken at the beginning of puberty. A simple rule is that, at the beginning of puberty, there is an average of 5 cm growth remaining at the knee. There are four common different scenarios: (1) A 5-cm discrepancy-epiphysiodesis of both femur and tibia at the beginning of puberty (11 years bone age girls and 13 years in boys). (2) A 4-cm discrepancy-epiphysiodesis of femur and tibia 6 months after the onset of puberty (11 years 6 months bone age girls, 13 years 6 months bone age boys, tri-radiate cartilage open). (3) A 3-cm discrepancy-epiphysiodesis of femur only at the start of puberty, (skeletal age of 11 years in girls and 13 years in boys). (4) A 2-cm discrepancy-epiphysiodesis of femur only, 1 year after the start of puberty (12 years bone age girls and 14 years in boys).
Figures





References
-
- Dimeglio A. La coissance en orthopedie. Montpellier: Sauramps; 1987.
-
- Dimeglio A. Growth in pediatric orthopaedics. J Pediatr Orthop. 2001;21(4):549–555. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
