

Adolescent patellofemoral pain: implicating the medial patellofemoral ligament as the main pain generator
- PMID: 19308554
- PMCID: PMC2656832
- DOI: 10.1007/s11832-008-0104-2
Adolescent patellofemoral pain: implicating the medial patellofemoral ligament as the main pain generator
Abstract
Purpose: The purpose of this study is to define the clinical presentation of adolescent patellofemoral pain.
Methods: A review was completed of all patients with patellofemoral pain at a children's hospital sports clinic over a 3-year period.
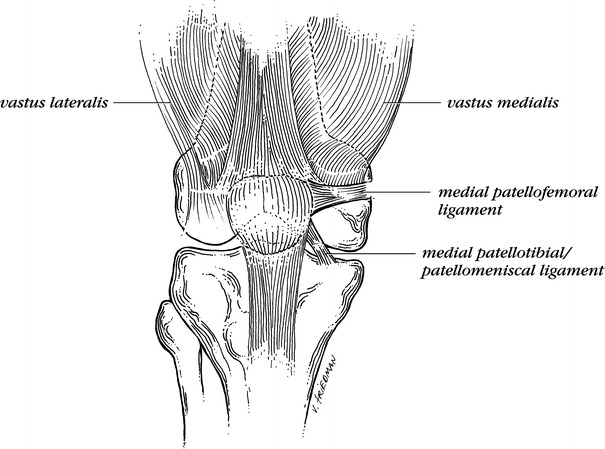
Results: One hundred and one patients (91 female) with 136 symptomatic knees were identified. Mean age was 14.4 years. Knee pain was localized to the anteromedial or anterior region of the knee in 96% of patients and was typically produced with running (94%), jumping (92%) and stair use (69%). On physical examination there was usually a non antalgic gait (99%), no patellofemoral crepitation (98%), normal lower extremity angular (84%) and rotational alignment (94%), with no foot malalignment (>97%). The medial patellofemoral ligament (MPFL) was the most palpably tender area of the knee in 98% of patients. During "lateral apprehension" testing, 89% had pain at the MPFL, but not true apprehension. A "J-sign" was present at terminal knee extension in 65%. Mean Q-angle was 18.7 degrees . Means of all radiographic measures were within normal ranges.
Conclusion: The prototypical patient had anterior/anteromedial knee pain of insidious onset during running and jumping. The most consistent physical findings were focal tenderness at the MPFL, positive terminal J-sign, and an elevated Q-angle. Most patients required only nonsurgical treatments, but 18% underwent surgical interventions for persistent pain.
Figures
References
-
- Ficat RP, Philippe J, Hungerford DS. Chondromalacia patellae: a system of classification. Clin Orthop. 1979;144:55–62. - PubMed
-
- Fulkerson JP. The etiology of patellofemoral pain in young, active patients: a prospective study. Clin Orthop. 1983;179:129–133. - PubMed
-
- Insall J, Falvo KA, Wise DW. Chondromalacia patellae. A prospective study. J Bone Joint Surg [Am] 1976;58:1–8. - PubMed
-
- Johnson RP. Lateral facet syndrome of the patella. Lateral restraint analysis and use of lateral resection. Clin Orthop. 1989;238:148–158. - PubMed
LinkOut - more resources
Full Text Sources
