

New classification and score for tibial hemimelia
- PMID: 19308574
- PMCID: PMC2656800
- DOI: 10.1007/s11832-008-0081-5
New classification and score for tibial hemimelia
Abstract
Purpose: Previous classifications of tibial malformations are no longer sufficient and practical for clinics and treatment. They are not precisely defined, include incorrect pathological-anatomical definitions, are related to X-ray diagnosis only, miss complete formal types of malformation, or describe too complex concepts not useful for clinical applications (Jones et al., J Bone Joint Surg B 60:31-39, 1978; Kalamchi and Dawe, J Bone Joint Surg B 67:581-584, 1985; Henkel et al., Arch Orthop Trauma Surg 93:1-19, 1978). More precise preoperative diagnosis, including by sonography and MRI and experienced intraoperative analysis of anatomical structures ensure exact description of the pathological-anatomical situation which can be used because of new potential in therapy. Until now, no score was available for detection of additional limb malformations and, therefore, clinical and scientific comparison of the different tibial reduction deficiencies, especially in respect to the success of therapy, was not sufficiently realisable. A new classification and score is presented reflecting the improved therapy currently available.
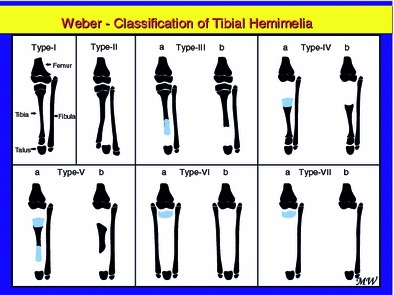
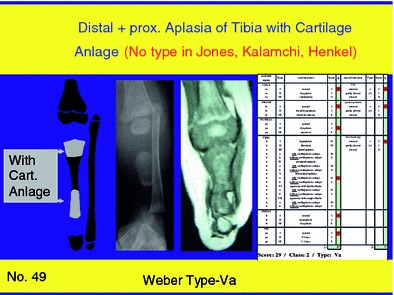
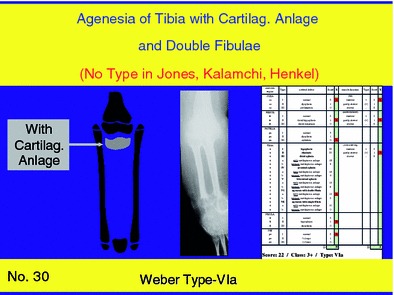
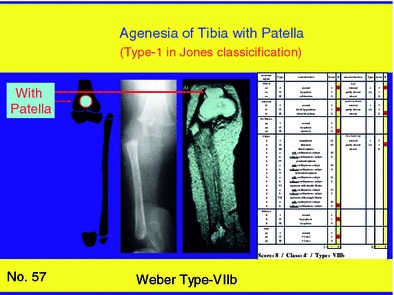
Methods: In this classification and score the main pathological findings of the complete leg are included (coxa-femur-patella-tibia-fibula-pes), with specific importance of the tibia. Tibial malformations are divided into seven main groups and five of them into two subgroups. The cartilaginous anlage of the tibia which has not yet received much attention in the literature plays an important role in this classification. Only seven main types of tibial defect have to be recognized and, if necessary, additional defects of the whole leg, including the function of the affected parts, can be summarized in a-five-class-system.
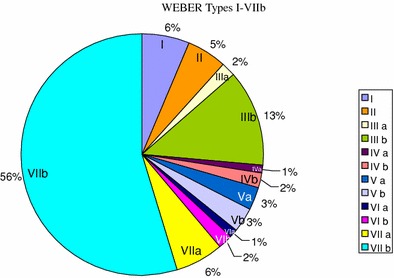
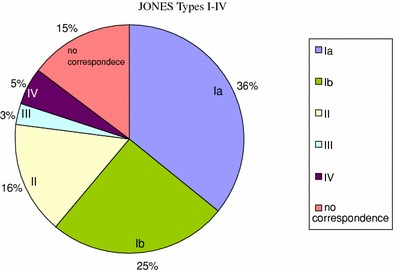
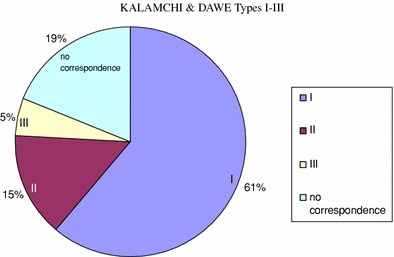
Results: With this classification and this score system which was evaluated on 95 affected limbs, with a sex ratio of 51%:49% (male:female), right:left affection, and unilateral:bilateral affection also, we found the sequence of the distribution of types as follows: 61% of cases with type-VII, 15% with type-III, 6% with type-I, 6% with type-V, 5% with type-II, 3% with type-IV, and 3% with type-VI. In comparison with the Jones et al. (J Bone Joint Surg B 60:31-39, 1978), Kalamchi and Dawe (J Bone Joint Surg B 67:581-584, 1985) and Henkel et al. (Arch Orthop Trauma Surg 93:1-19, 1978) classifications the tibial defects in the presented classification are detected more precisely, the pathological anatomical terms are correctly used, the whole leg and all main functions are included and, thus, reference to therapeutical possibilities is given.
Conclusions: The new classification and the score system allow simple, therapeutically relevant, and comprehensive classification and, additionally, scientific comparison of the different pattern of defects described by diverse authors. For daily clinical use the tibial classification only is preferred.
Figures
Similar articles
-
Systematic radiographic evaluation of tibial hemimelia with orthopedic implications.Pediatr Radiol. 2017 Apr;47(4):473-483. doi: 10.1007/s00247-016-3730-8. Epub 2017 Jan 3. Pediatr Radiol. 2017. PMID: 28050636 Review.
-
Occurrence of Malformations of the Upper Extremity in Tibial Hemimelia: Correlation with the Jones Classification.Indian J Orthop. 2025 Mar 21;59(5):650-658. doi: 10.1007/s43465-025-01359-9. eCollection 2025 May. Indian J Orthop. 2025. PMID: 40321490 Free PMC article.
-
[Clubfoot associated with tibial and fibular hemimelia].Z Orthop Unfall. 2012 Oct;150(5):525-32. doi: 10.1055/s-0032-1314997. Epub 2012 Oct 17. Z Orthop Unfall. 2012. PMID: 23076751 German.
-
Femoral bifurcation and bilateral tibial hemimelia: case report.Pan Afr Med J. 2018 Jun 5;30:99. doi: 10.11604/pamj.2018.30.99.11969. eCollection 2018. Pan Afr Med J. 2018. PMID: 30344883 Free PMC article.
-
Screening for extermity arterial injury with the arterial pressure index.Am J Emerg Med. 2005 Sep;23(5):689-95. doi: 10.1016/j.ajem.2004.12.013. Am J Emerg Med. 2005. PMID: 16140180 Review.
Cited by
-
Physiolysis for Metatarsal Bracketed Epiphysis.J Pediatr Soc North Am. 2024 Feb 5;5(4):773. doi: 10.55275/JPOSNA-2023-773. eCollection 2023 Nov. J Pediatr Soc North Am. 2024. PMID: 40432945 Free PMC article.
-
Bilateral Calcaneus Transfers for the Treatment of Congenital Tibial Deficiencies: A Novel Surgical Technique and Case Report.J Am Acad Orthop Surg Glob Res Rev. 2022 Dec 5;6(12):e22.00070. doi: 10.5435/JAAOSGlobal-D-22-00070. eCollection 2022 Dec 1. J Am Acad Orthop Surg Glob Res Rev. 2022. PMID: 36732306 Free PMC article.
-
Systematic radiographic evaluation of tibial hemimelia with orthopedic implications.Pediatr Radiol. 2017 Apr;47(4):473-483. doi: 10.1007/s00247-016-3730-8. Epub 2017 Jan 3. Pediatr Radiol. 2017. PMID: 28050636 Review.
-
GLI3: a mediator of genetic diseases, development and cancer.Cell Commun Signal. 2020 Apr 3;18(1):54. doi: 10.1186/s12964-020-00540-x. Cell Commun Signal. 2020. PMID: 32245491 Free PMC article. Review.
-
Tibial hemimelia associated with GLI3 truncation.J Hum Genet. 2016 May;61(5):443-6. doi: 10.1038/jhg.2015.161. Epub 2016 Jan 21. J Hum Genet. 2016. PMID: 26791356
References
-
- Billroth T. Ueber einige durch Knochendefecte bedingte Krümmungen des Fusses. Arch Klin Chir. 1861;1:252–268.
-
- Dankmeijer J. Congenital absence of the tibia. Anat Rec. 1935;62:179–194. doi: 10.1002/ar.1090620205. - DOI
-
- Brown FW. The brown operation for total hemimelia tibia. In: Aitken GT, editor. Selected lower-limb anomalies. Washington: National Academy of Sciences; 1971. pp. 20–28.
-
- Jones D, Barnes J, Lloyd-Roberts GC. Congenital aplasia and dysplasia of the tibia with intact fibula: classification and management. J Bone Joint Surg B. 1978;60:31–39. - PubMed
LinkOut - more resources
Full Text Sources
