

One-stage hip reconstruction in late neglected developmental dysplasia of the hip presenting in children above 8 years of age
- PMID: 19308607
- PMCID: PMC2656836
- DOI: 10.1007/s11832-008-0135-8
One-stage hip reconstruction in late neglected developmental dysplasia of the hip presenting in children above 8 years of age
Abstract
Purpose: To assess the clinical and radiological results of one-stage hip reconstruction for late neglected developmental dysplasia of the hip (DDH) in children above 8 years of age.
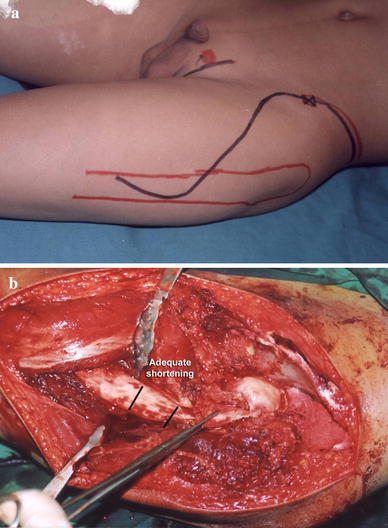
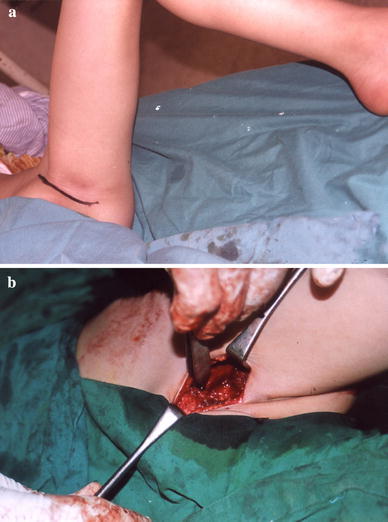
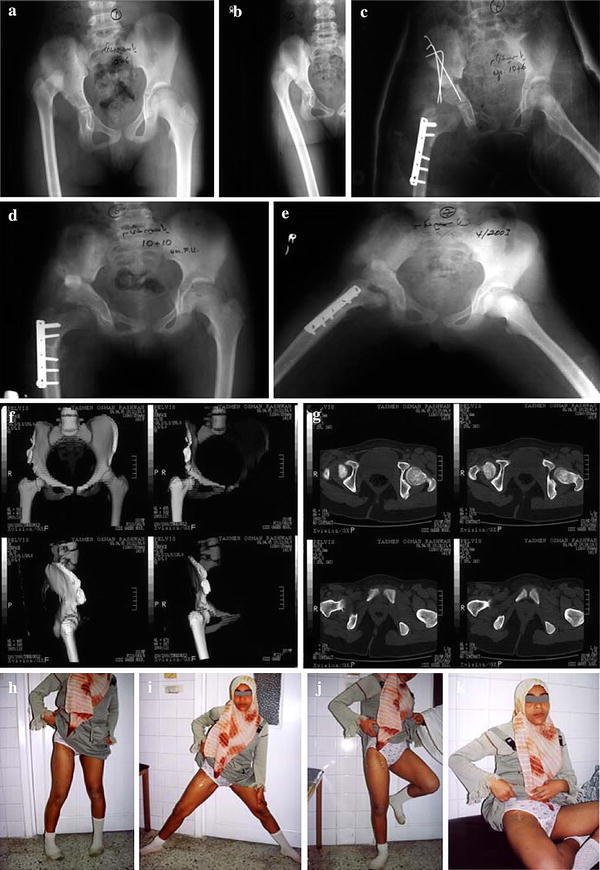
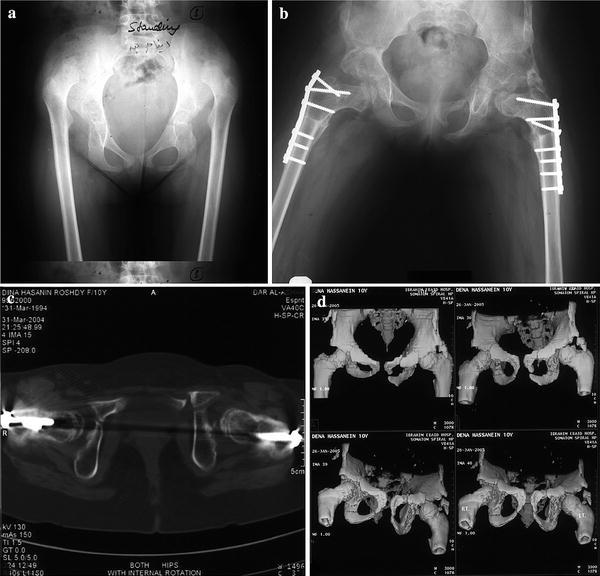
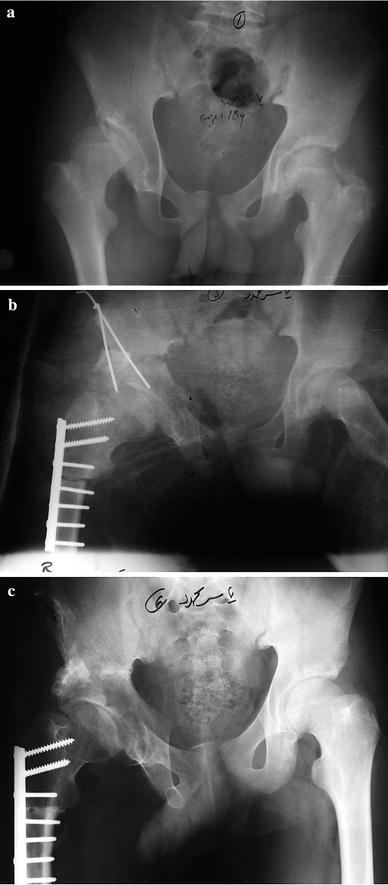
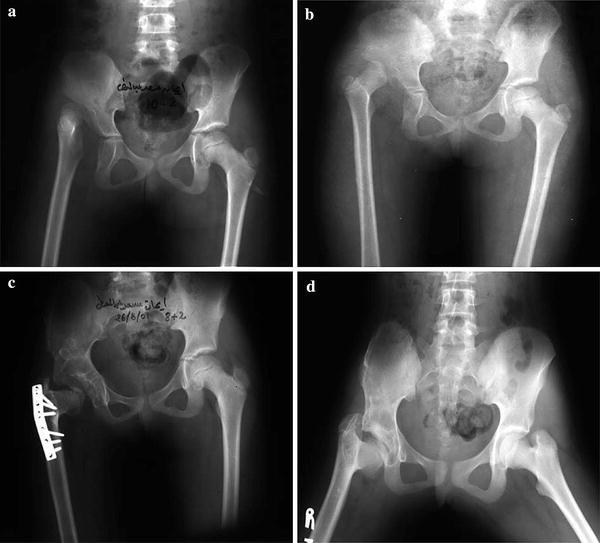
Methods: Nineteen hips in 16 patients, 14 females and two males (three being bilateral), were treated by open reduction adequate shortening (up to 5 cm) with derotation, and limited varization if needed, tight capsulorrhaphy, and appropriate pelvic reconstruction (Salter or triple acetabular osteotomy). The average age at operation 10.6 years (range 8-18 years). The period of follow up ranged from 3 to 9 years. A modified approach for the hip joint and upper femur was utilized, allowing better exposure. Pre- and post-operative plain radiography was performed for all cases and at follow up. Computed tomography (CT) or multislice CT with 3D reconstruction were carried out pre-operatively for recent cases and post-operatively for all, and were found to be helpful in providing a panorama of the dysplastic hip and in planning the required surgery and assessing the results.
Results: According to the McKay modified criteria, 15 hips (79%) were clinically excellent to good, while four hips (21%) were fair to poor. Radiographically, according to the Severin modified criteria, 16 hips (84%) were excellent to good and three hips (16%) were fair to poor. Limb length discrepancy ranged from 0.5 to 2.1 cm, as measured by CT scanograms. Complications were avascular necrosis (AVN) in an early case due to limited femoral shortening with resultant excessive stress over the femoral head and subluxation in another case.
Conclusion: A one-stage hip reconstruction for late neglected cases of DDH have achieved excellent results if adequate shortening with derotation is performed, together with appropriate acetabular reconstruction and tight capsulorrhaphy. Varization should not replace part or all of the required shortening, and should be added if required.
Figures


References
-
- Ashley RK, Larsen LJ, James PM. Reduction of dislocation of the hip in older children: a preliminary report. J Bone Joint Surg Am. 1972;54:545–550. - PubMed
-
- Berkeley ME, Dickson JH, Cain TE, Donovan MM. Surgical therapy for congenital dislocation of the hip in patients who are twelve to thirty-six months old. J Bone Joint Surg Am. 1984;66:412–420. - PubMed
-
- Coleman SS. Congenital dysplasia and dislocation of the hip. St. Louis, MO: CV Mosby; 1978. pp. 95–154.
-
- Lindstrom JR, Ponseti IV, Wenger DR. Acetabular development after reduction in congenital dislocation of the hip. J Bone Joint Surg Am. 1979;61:112–118. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
