

Angiographic and clinical outcomes of drug-eluting versus bare metal stent deployment in the Occluded Artery Trial
- PMID: 19309733
- PMCID: PMC2819385
- DOI: 10.1002/ccd.21930
Angiographic and clinical outcomes of drug-eluting versus bare metal stent deployment in the Occluded Artery Trial
Abstract
Background: The majority of patients randomized to percutaneous coronary intervention (PCI) in the Occluded Artery Trial (OAT) and its angiographic substudy, the Total Occlusion Study of Canada 2 (TOSCA-2) were treated with bare metal stents (BMS). We aimed to determine if stenting of the target occlusion in OAT with drug-eluting stents (DES) was associated with more favorable angiographic results and clinical outcome when compared with treatment with BMS.
Methods: TOSCA-2 DES was a prospective nonrandomized substudy that provided 1-year angiographic comparison of late loss and reocclusion in 25 patients treated with DES and in 128 treated with BMS. In addition, all PCI-assigned patients enrolled from the time when DES were first utilized were similarly categorized (DES n = 77, and BMS n = 386) and compared using the 3-year cumulative OAT primary combined endpoint of death, myocardial infarction, or Class-IV heart failure, as well as angina.
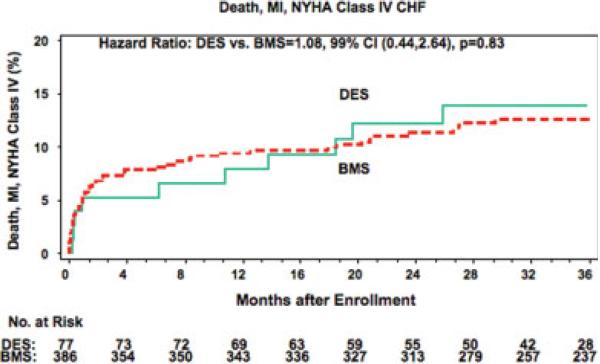
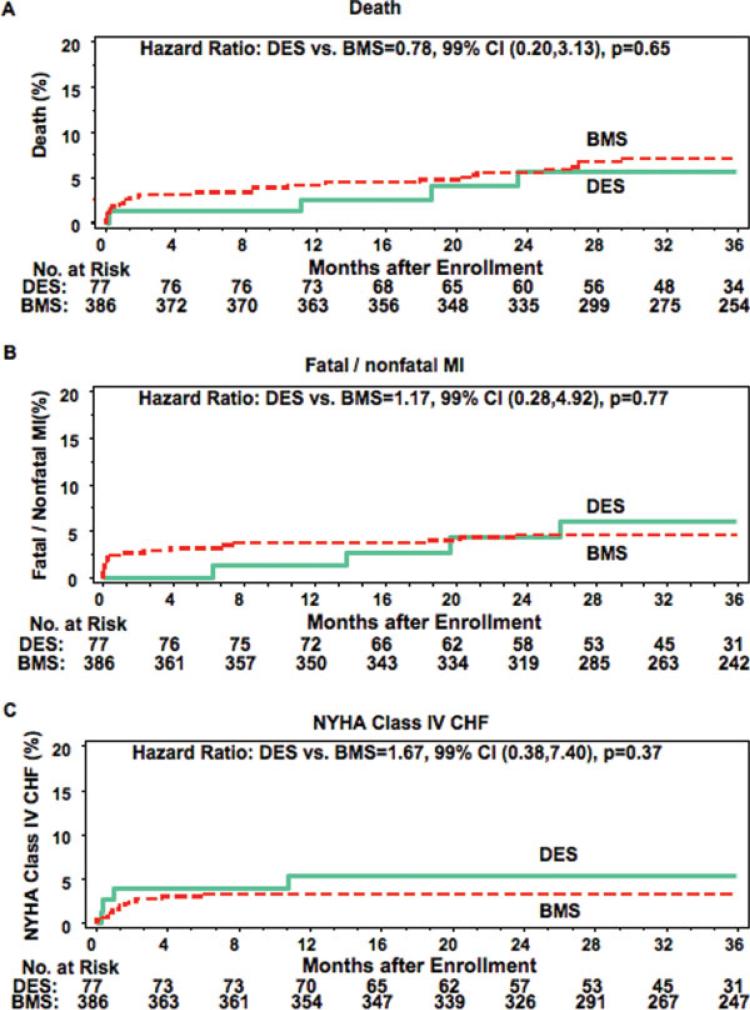
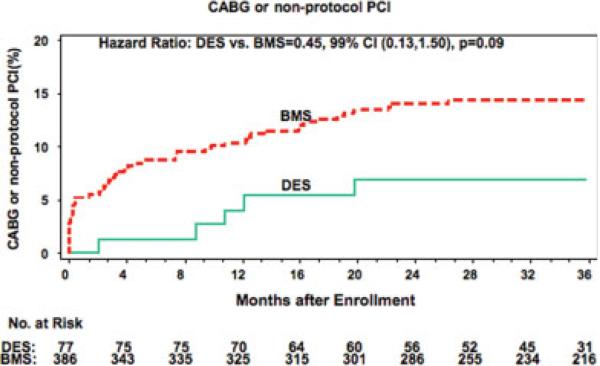
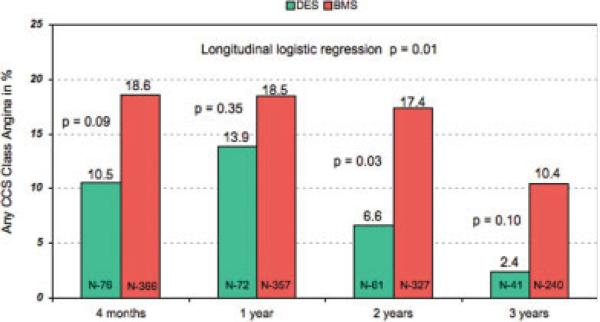
Results: In-segment late loss was 0.14 +/- 0.45 mm for DES and 0.75 +/- 0.86 mm for BMS (P < 0.001). Corresponding binary restenosis rates were 13.0% and 44.3% (P = 0.005). Occlusion at 1 year was observed in 4.0 and 12.1%, respectively (P = 0.23). The 3-year cumulative primary event rate was 13.8% with DES and 12.5% with BMS (hazard ratio 1.08, 99% confidence intervals 0.44, 2.64; P = 0.83). Angina over time occurred less frequently in the DES group (P = 0.01).
Conclusions: Although the reduction of late loss and trend to reduction in reocclusion with the use of DES for PCI of persistently occluded IRA 3-28 days post myocardial infarction did not translate into a signal for reduction in death, reinfarction, or Class IV heart failure, DES use was associated with less angina over time. Further follow-up is warranted.
Figures
Comment in
-
DES in CTO: cosmetic or clinical benefit.Catheter Cardiovasc Interv. 2009 May 1;73(6):780. doi: 10.1002/ccd.22060. Catheter Cardiovasc Interv. 2009. PMID: 19370758 No abstract available.
References
-
- Dzavik V, Buller CE, Lamas GA, et al. Randomized trial of percutaneous coronary intervention for subacute infarct-related coronary artery occlusion to achieve long-term patency and improve ventricular function: The total occlusion study of Canada (TOSCA)-2 trial. Circulation. 2006;114:2449–2457. - PMC - PubMed
-
- Rubartelli P, Niccoli L, Verna E, Giachero C, Zimarino M, Fontanelli A, Vassanelli C, Campolo L, Martuscelli E, Tommasini G. Stent implantation versus balloon angioplasty in chronic coronary occlusions: Results from the GISSOC trial. Gruppo Italiano di Studio sullo Stent nelle Occlusioni Coronariche. J Am Coll Cardiol. 1998;32:90–96. - PubMed
-
- Sirnes PA, Golf S, Myreng Y, Molstad P, Emanuelsson H, Albertsson P, Brekke M, Mangschau A, Endresen K, Kjekshus J. Stenting in chronic coronary occlusion (SICCO): A randomized, controlled trial of adding stent implantation after successful angioplasty. J Am Coll Cardiol. 1996;28:1444–1451. - PubMed
-
- Hochman JS, Lamas GA, Knatterud GL, Buller CE, Dzavik V, Mark DB, Reynolds HR, White HD. Design and methodology of the occluded artery trial (OAT). Am Heart J. 2005;150:627–642. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
