

Comparison of CD4 cell count, viral load, and other markers for the prediction of mortality among HIV-1-infected Kenyan pregnant women
- PMID: 19317628
- PMCID: PMC2758232
- DOI: 10.1086/597617
Comparison of CD4 cell count, viral load, and other markers for the prediction of mortality among HIV-1-infected Kenyan pregnant women
Abstract
Background: There are limited data regarding the relative merits of biomarkers as predictors of mortality or time to initiation of antiretroviral therapy (ART).
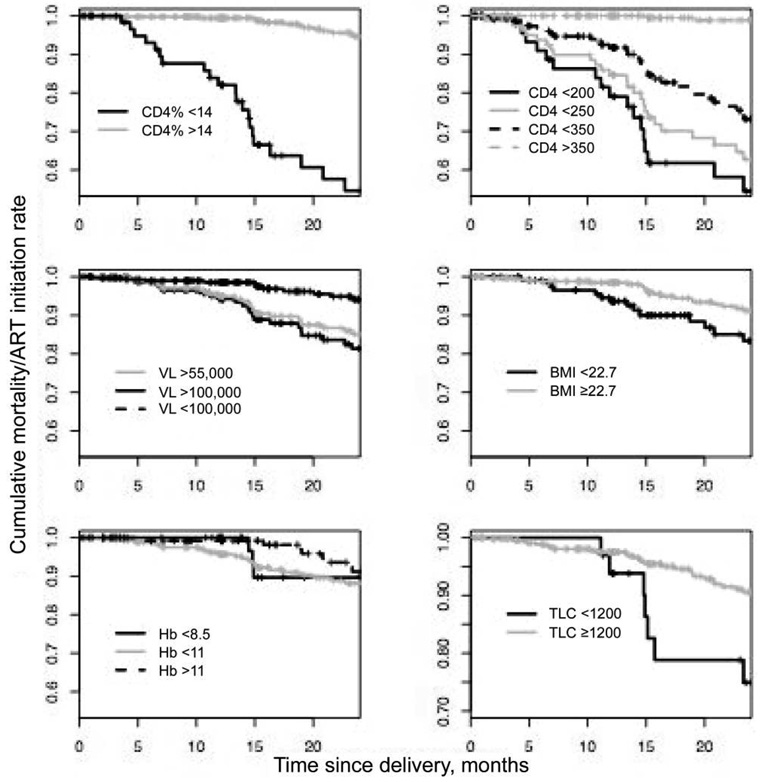
Methods: We evaluated the usefulness of the CD4 cell count, CD4 cell percentage (CD4%), human immunodeficiency virus type 1 (HIV-1) load, total lymphocyte count (TLC), body mass index (BMI), and hemoglobin measured at 32 weeks' gestation as predictors of mortality in a cohort of HIV-1-infected women in Nairobi, Kenya. Sensitivity, specificity, positive predictive value (PPV), and area under the receiver operating characteristic (ROC) curve (AUC) were determined for each biomarker separately, as well as for the CD4 cell count and the HIV-1 load combined.
Results: Among 489 women with 10,150 person-months of follow-up, mortality rates at 1 and 2 years postpartum were 2.1% (95% confidence interval [CI], 0.7%-3.4%) and 5.5% (95% CI, 3.0%-8.0%), respectively. CD4 cell count and CD4% had the highest AUC value (>0.9). BMI, TLC, and hemoglobin were each associated with but poorly predictive of mortality (PPV, <7%). The HIV-1 load did not predict mortality beyond the CD4 cell count.
Conclusions: The CD4 cell count and CD4% measured during pregnancy were both useful predictors of mortality among pregnant women. TLC, BMI, and hemoglobin had a limited predictive value, and the HIV-1 load did not predict mortality any better than did the CD4 cell count alone.
Conflict of interest statement
Potential conflicts of interest: none reported.
Figures



Comment in
-
Monitoring HIV treatment in resource-limited settings: reassuring news on the usefulness of CD4(+) cell counts.J Infect Dis. 2009 May 1;199(9):1255-7. doi: 10.1086/597618. J Infect Dis. 2009. PMID: 19317627 No abstract available.
References
-
- World Health Organization/Joint United Nations Programme on HIV/AIDS/United Nations Children’s Fund. Towards universal access: scaling up priority HIV/AIDS interventions in the health sector: progress report. 2007. Apr [Accessed 10 October 2007]. Available at: http://www.who.int/hiv/mediacentre/universal_access_progress_report_en.pdf.
-
- Ekouevi DK, Inwoley A, Tonwe-Gold B, et al. Variation of CD4 count and percentage during pregnancy and after delivery: implications for HAART initiation in resource-limited settings. AIDS Res Hum Retroviruses. 2007;23:1469–1473. - PubMed
-
- Mulcahy F, Wallace E, Woods S, et al. Counts in pregnancy do not accurately reflect the need for long-term HAART [abstract 704b]. Program and abstracts of the 13th Conference on Retroviruses and Opportunistic Infections (Denver); 2006. Available at: http://www.retroconference.org/2006/Abstracts/27587.htm.
-
- Miotti PG, Liomba G, Dallabetta GA, Hoover DR, Chiphangwi JD, Saah AJ. T lymphocyte subsets during and after pregnancy: analysis in human immunodeficiency virus type 1–infected and –uninfected Malawian mothers. J Infect Dis. 1992;165:1116–1119. - PubMed
-
- Temmerman M, Nagelkerke N, Bwayo J, Chomba EN, Ndinya-Achola J, Piot P. HIV-1 and immunological changes during pregnancy: a comparison between HIV-1-seropositive and HIV-1-seronegative women in Nairobi, Kenya. AIDS. 1995;9:1057–1060. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
