

Association of HIV viral load with monocyte chemoattractant protein-1 and atherosclerosis burden measured by magnetic resonance imaging
- PMID: 19318907
- PMCID: PMC2786203
- DOI: 10.1097/QAD.0b013e328329c76b
Association of HIV viral load with monocyte chemoattractant protein-1 and atherosclerosis burden measured by magnetic resonance imaging
Abstract
Background: HIV-infected individuals may be at increased risk for atherosclerosis. Although this is partially attributable to metabolic factors, HIV-associated inflammation may play a role.
Objective: To investigate associations of HIV disease with serum monocyte chemoattractant protein-1/chemokine (C-C motif) ligand 2 (MCP-1/CCL2) levels and atherosclerosis burden.
Design: A cross-sectional analysis.
Methods: : Serum MCP-1/CCL2, fasting lipids, and glucose tolerance were measured in 98 HIV-infected and 79 demographically similar uninfected adults. Eighty-four participants had MRI of the carotid arteries and thoracic aorta to measure atherosclerosis burden. Multivariate analyses were performed using linear regression.
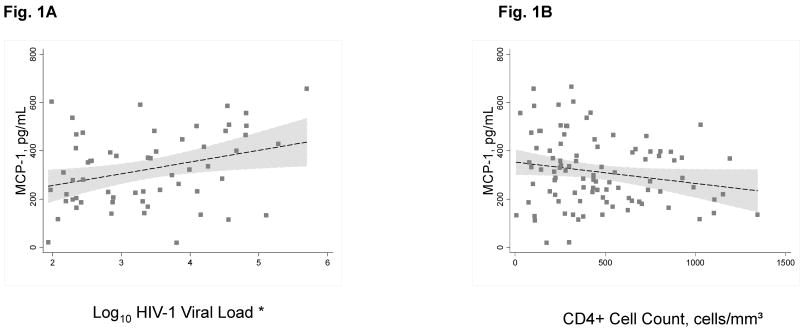
Results: Mean MCP-1/CCL2 levels did not differ between HIV-infected and uninfected participants (P = 0.65). Among HIV-infected participants, after adjusting for age, BMI, and cigarette smoking, HIV-1 viral load was positively associated with MCP-1/CCL2 (P = 0.02). Multivariate analyses adjusting for sex, low-density lipoprotein cholesterol, total cholesterol:high-density lipoprotein cholesterol ratio, cigarette smoking, MCP-1/CCL2, and protease inhibitor use found that HIV infection was associated with greater mean thoracic aorta vessel wall area (VWA, P < 0.01) and vessel wall thickness (VWT, P = 0.03), but not with carotid artery parameters. Compared with being uninfected, having detectable HIV-1 viremia was associated with greater mean thoracic aorta VWA (P < 0.01) and VWT (P = 0.03), whereas being HIV-infected with undetectable viral load was associated with greater thoracic aorta VWA (P = 0.02) but not VWT (P = 0.15). There was an independent positive association of MCP-1/CCL2 with thoracic aorta VWA (P = 0.01) and VWT (P = 0.01).
Conclusion: HIV-1 viral burden is associated with higher serum levels of MCP-1/CCL2 and with atherosclerosis burden, as assessed by thoracic aorta VWA and VWT.
Conflict of interest statement
Figures

Similar articles
-
Carotid magnetic resonance imaging in persons living with HIV and 10-year atherosclerotic cardiovascular disease risk score.Antivir Ther. 2018;23(8):695-698. doi: 10.3851/IMP3258. Antivir Ther. 2018. PMID: 30088806
-
Nonconcordance between subclinical atherosclerosis and the calculated Framingham risk score in HIV-infected patients: relationships with serum markers of oxidation and inflammation.HIV Med. 2010 Apr;11(4):225-31. doi: 10.1111/j.1468-1293.2009.00766.x. Epub 2009 Oct 21. HIV Med. 2010. PMID: 19845792
-
Metabolic abnormalities and viral replication are associated with biomarkers of vascular dysfunction in HIV-infected children.HIV Med. 2012 May;13(5):264-75. doi: 10.1111/j.1468-1293.2011.00970.x. Epub 2011 Dec 4. HIV Med. 2012. PMID: 22136114 Free PMC article.
-
Circulating Monocyte Chemoattractant Protein-1 and Risk of Stroke: Meta-Analysis of Population-Based Studies Involving 17 180 Individuals.Circ Res. 2019 Sep 27;125(8):773-782. doi: 10.1161/CIRCRESAHA.119.315380. Epub 2019 Sep 3. Circ Res. 2019. PMID: 31476962 Free PMC article.
-
Monocyte chemoattractant protein-1/CCL2 as a biomarker in acute coronary syndromes.Curr Atheroscler Rep. 2009 Mar;11(2):131-8. doi: 10.1007/s11883-009-0021-y. Curr Atheroscler Rep. 2009. PMID: 19228487 Free PMC article. Review.
Cited by
-
Non-classical monocytes predict progression of carotid artery bifurcation intima-media thickness in HIV-infected individuals on stable antiretroviral therapy.HIV Clin Trials. 2016 May;17(3):114-22. doi: 10.1080/15284336.2016.1162386. Epub 2016 Apr 4. HIV Clin Trials. 2016. PMID: 27125366 Free PMC article.
-
The deleterious influence of tenofovir-based therapies on the progression of atherosclerosis in HIV-infected patients.Mediators Inflamm. 2012;2012:372305. doi: 10.1155/2012/372305. Epub 2012 May 7. Mediators Inflamm. 2012. PMID: 22645407 Free PMC article.
-
HIV infection and stroke: current perspectives and future directions.Lancet Neurol. 2012 Oct;11(10):878-90. doi: 10.1016/S1474-4422(12)70205-3. Lancet Neurol. 2012. PMID: 22995692 Free PMC article. Review.
-
Inflammatory biomarkers and subclinical carotid atherosclerosis in HIV-infected and HIV-uninfected men in the Multicenter AIDS Cohort Study.PLoS One. 2019 Apr 4;14(4):e0214735. doi: 10.1371/journal.pone.0214735. eCollection 2019. PLoS One. 2019. PMID: 30946765 Free PMC article.
-
Subclinical Atherosclerosis Imaging in People Living with HIV.J Clin Med. 2019 Jul 29;8(8):1125. doi: 10.3390/jcm8081125. J Clin Med. 2019. PMID: 31362391 Free PMC article. Review.
References
-
- Stein JH, Klein MA, Bellehumeur JL, McBride PE, Wiebe DA, Otvos JD, et al. Use of human immunodeficiency virus-1 protease inhibitors is associated with atherogenic lipoprotein changes and endothelial dysfunction. Circulation. 2001;104:257–262. - PubMed
-
- Anastos K, Lu D, Shi Q, Tien PC, Kaplan RC, Hessol NA, et al. Association of serum lipid levels with HIV serostatus, specific antiretroviral agents, and treatment regimens. J Acquir Immune Defic Syndr. 2007;45:34–42. - PubMed
-
- Samaras K, Wand H, Law M, Emery S, Cooper D, Carr A. Prevalence of metabolic syndrome in HIV-infected patients receiving highly active antiretroviral therapy using International Diabetes Foundation and Adult Treatment Panel III criteria: associations with insulin resistance, disturbed body fat compartmentalization, elevated C-reactive protein, and [corrected] hypoadiponectinemia. Diabetes Care. 2007;30:113–119. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL073458/HL/NHLBI NIH HHS/United States
- R01 DA013564/DA/NIDA NIH HHS/United States
- K12 RR017672/RR/NCRR NIH HHS/United States
- L30 DA017071/DA/NIDA NIH HHS/United States
- P30 AI051519/AI/NIAID NIH HHS/United States
- K12-RR1767203/RR/NCRR NIH HHS/United States
- R01 HL071021/HL/NHLBI NIH HHS/United States
- R01 DA014998/DA/NIDA NIH HHS/United States
- R01 DA14998/DA/NIDA NIH HHS/United States
- R01 MH075679/MH/NIMH NIH HHS/United States
- M01-RR12248/RR/NCRR NIH HHS/United States
- R01 MH070297/MH/NIMH NIH HHS/United States
- MH075679/MH/NIMH NIH HHS/United States
- MH070297/MH/NIMH NIH HHS/United States
- M01 RR012248/RR/NCRR NIH HHS/United States
- R01 DA13564/DA/NIDA NIH HHS/United States
- 5 P30AI-051519/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
