

A pilot asthma incidence surveillance system and case definition: lessons learned
- PMID: 19320369
- PMCID: PMC2646484
- DOI: 10.1177/003335490912400215
A pilot asthma incidence surveillance system and case definition: lessons learned
Abstract
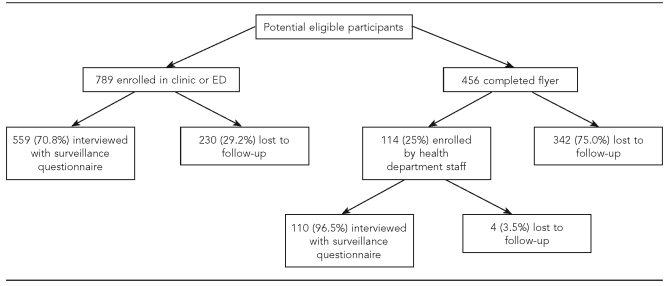
Objectives: Surveillance for incident asthma in the general population could provide timely information about asthma trends and new, emerging etiologic factors. We sought to determine the feasibility of an asthma incidence surveillance system using voluntary reporting of asthma by outpatient clinics and emergency departments (EDs).
Methods: Voluntary reporting occurred from July 2002 through June 2006. We classified reported asthma based on a case definition adapted from one developed by the Council of State and Territorial Epidemiologists. We validated the case definition by having pulmonologists review data from participant interviews, medical record abstractions, and pulmonary function test (PFT) results.
Results: The positive predictive value (PPV) of meeting any of the case definition criteria for asthma was 80% to 82%. The criterion of taking at least one rescue and one controller medication had the highest PPV (97% to 100%). Only 7% of people meeting the incident case definition had a PFT documented in their medical record, limiting the usefulness of PFT results for case classification. Compared with pediatric participants, adult participants were more likely to be uninsured and to obtain asthma care at EDs. The surveillance system cost $5129 per enrolled person meeting the incident case definition and was difficult to implement in participating clinics and EDs because asthma reporting was not mandatory and informed consent was necessary.
Conclusions: The project was useful in evaluating the case definition's validity and in describing the participants' characteristics and health-care use patterns. However, without mandatory reporting laws, reporting of incident asthma in the general population by clinicians is not likely to be a feasible method for asthma surveillance.
Figures
References
-
- Moorman JE, Rudd RA, Johnson CA, King M, Minor P, Bailey C, et al. National surveillance for asthma—United States, 1980–2004. MMWR Surveill Summ. 2007;56(8):1–54. - PubMed
-
- Weiss KB, Sullivan SD. The health economics of asthma and rhinitis. I. Assessing the economic impact. J Allergy Clin Immunol. 2001;107:3–8. - PubMed
-
- Thacker SB. Historical development. In: Teutsch SM, Churchill RE, editors. Principles and practice of public health surveillance. 2nd ed. New York: Oxford University Press; 2000. pp. 1–14.
