

Treatment center and geographic variability in pre-ESRD care associate with increased mortality
- PMID: 19321704
- PMCID: PMC2678038
- DOI: 10.1681/ASN.2008060624
Treatment center and geographic variability in pre-ESRD care associate with increased mortality
Abstract
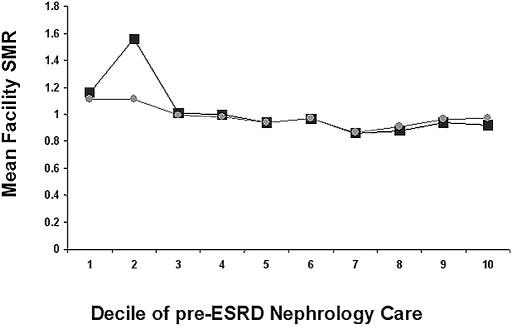
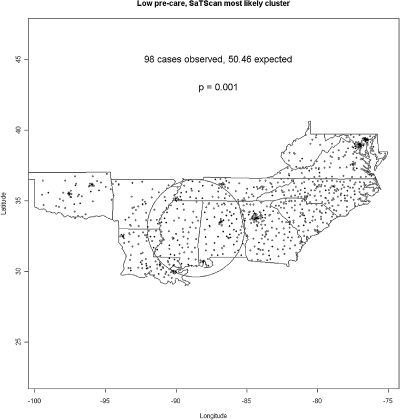
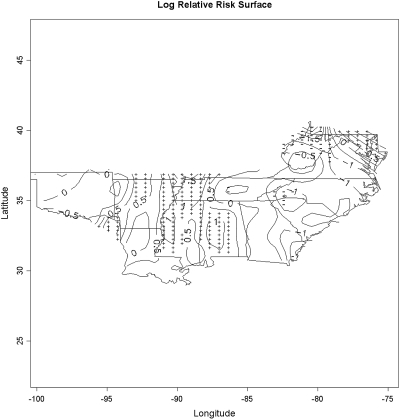
Late referral of patients with chronic kidney disease is associated with increased morbidity and mortality, but the contribution of center-to-center and geographic variability of pre-ESRD nephrology care to mortality of patients with ESRD is unknown. We evaluated the pre-ESRD care of > 30,000 incident hemodialysis patients, 5088 (17.8%) of whom died during follow-up (median 365 d). Approximately half (51.3%) of incident patients had received at least 6 mo of pre-ESRD nephrology care, as reported by attending physicians. Pre-ESRD nephrology care was independently associated with survival (odds ratio 1.54; 95% confidence interval 1.45 to 1.64). There was substantial center-to-center variability in pre-ESRD care, which was associated with increased facility-specific death rates. As the proportion of patients who were in a treatment center and receiving pre-ESRD nephrology care increased from lowest to highest quintile, the mortality rate decreased from 19.6 to 16.1% (P = 0.0031). In addition, treatment centers in the lowest quintile of pre-ESRD care were clustered geographically. In conclusion, pre-ESRD nephrology care is highly variable among treatment centers and geographic regions. Targeting these disparities could have substantial clinical impact, because the absence of > or = 6 mo of pre-ESRD care by a nephrologist is associated with a higher risk for death.
Figures
Comment in
-
Lessons from geographic variations in predialysis nephrology care.J Am Soc Nephrol. 2009 May;20(5):930-2. doi: 10.1681/ASN.2009030318. Epub 2009 Apr 23. J Am Soc Nephrol. 2009. PMID: 19389840 No abstract available.
References
-
- Ifudu O, Dawood M, Homel P, Friedman EA: Excess morbidity in patients starting uremia therapy without prior care by a nephrologist. Am J Kidney Dis 28: 841–845, 1996 - PubMed
-
- Obrador GT, Pereira BJ: Early referral to the nephrologist and timely initiation of renal replacement therapy: A paradigm shift in the management of patients with chronic renal failure. Am J Kidney Dis 31: 398–417, 1998 - PubMed
-
- Goransson LG, Bergrem H: Consequences of late referral of patients with end-stage renal disease. J Intern Med 250: 154–159, 2001 - PubMed
-
- Fink J, Blahut S, Reddy M, Light P: Use of erythropoietin before the initiation of dialysis and its impact on mortality. Am J Kidney Dis 37: 348–355, 2001 - PubMed
-
- Avorn J, Winkelmayer WC, Bohn RL, Levin R, Glynn RJ, Levy E, Owen W Jr: Delayed nephrologist referral and inadequate vascular access in patients with advanced chronic kidney failure. J Clin Epidemiol 55: 711–716, 2002 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
