

Esophagectomy for T1 esophageal cancer: outcomes in 100 patients and implications for endoscopic therapy
- PMID: 19324126
- PMCID: PMC2912110
- DOI: 10.1016/j.athoracsur.2008.12.060
Esophagectomy for T1 esophageal cancer: outcomes in 100 patients and implications for endoscopic therapy
Abstract
Objectives: Esophagectomy is the standard treatment for T1 esophageal cancer (EC). Interest in endoscopic therapies, particularly for T1 EC, is increasing. We evaluated the long-term outcomes after esophagectomy and examined the pathologic features of T1 cancer to determine the suitability for potential endoscopic therapy.
Methods: We reviewed the outcomes of esophagectomy in 100 consecutive patients with T1 EC. The primary end points studied were overall survival (OS) and disease-free survival (DFS). In addition to detailed pathology review, we evaluated prognostic variables associated with survival.
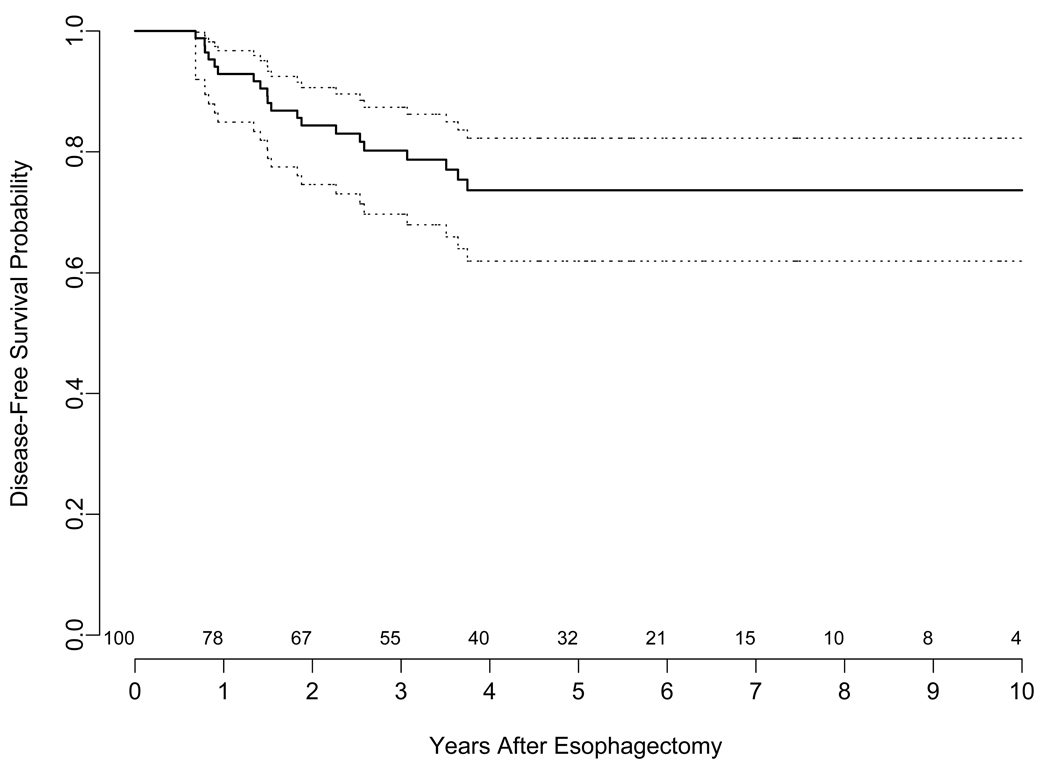
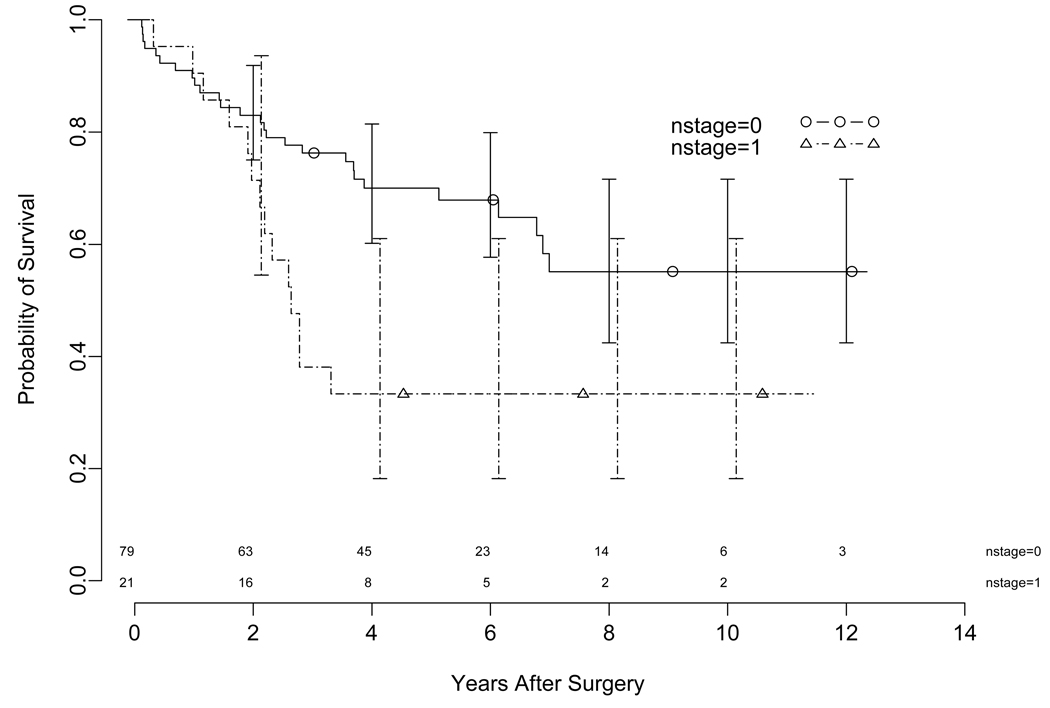
Results: Esophagectomy was performed in 100 patients (79 men, 21 women; median age, 68 years) for T1 EC, comprising adenocarcinoma, 91; squamous, 9; intramucosal (T1a), 29; and submucosal (T1b), 71. The 30-day mortality was 0%. Resection margins were microscopically negative in 99 patients (99%). N1 disease was present in 21 (T1a, 2 of 29 [7%]; T1b, 19 of 71 [27%]), associated high-grade dysplasia in 64 (64%), and angiolymphatic invasion in 19 (19%). At a median follow-up of 66 months, estimated 5-year OS was 62% and 3-year DFS was 80% for all patients (including N1). Nodal status and tumor size were significantly associated with OS and DFS, respectively.
Conclusions: Esophagectomy can be performed safely in patients with T1 EC with good long-term results. Many patients with T1 EC have several risk factors that may preclude adequate treatment with endoscopic therapy. Further prospective studies are required to evaluate endoscopic therapies. Esophagectomy should continue to remain the standard treatment in patients with T1 EC.
Figures

References
-
- Enzinger PC, Mayer RJ. Esophageal Cancer. N Engl J Med. 2003;349(23):2241–2252. - PubMed
-
- Rice TW, Blackstone EH, Goldblum JR, et al. Superficial adenocarcinoma of the esophagus. J Thorac Cardiovasc Surg. 2001 Dec;122(6):1077–1090. - PubMed
-
- Pennathur A, Landreneau RJ, Luketich JD. Surgical aspects of the patient with high-grade dysplasia. Semin Thorac Cardiovasc Surg. 2005;17(4):326–332. - PubMed
-
- Vieth M, Ell C, Gossner L, May A, Stolte M. Histological analysis of endoscopic resection specimens from 326 patients with Barrett's esophagus and early neoplasia. Endoscopy. 2004 Sep;36(9):776–781. - PubMed
-
- Ell C, May A, Pech O, et al. Curative endoscopic resection of early esophageal adenocarcinomas (Barrett's cancer) Gastrointest Endosc. 2007 Jan;65(1):3–10. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
