

Pulmonary hypertension in heart failure with preserved ejection fraction: a community-based study
- PMID: 19324256
- PMCID: PMC2736110
- DOI: 10.1016/j.jacc.2008.11.051
Pulmonary hypertension in heart failure with preserved ejection fraction: a community-based study
Abstract
Objectives: This study sought to define the prevalence, severity, and significance of pulmonary hypertension (PH) in heart failure with preserved ejection fraction (HFpEF) in the general community.
Background: Although HFpEF is known to cause PH, its development is highly variable. Community-based data are lacking, and the relative contribution of pulmonary venous versus pulmonary arterial hypertension (HTN) to PH in HFpEF is unknown. We hypothesized that PH would be a marker of symptomatic pulmonary congestion, distinguishing HFpEF from pre-clinical hypertensive heart disease.
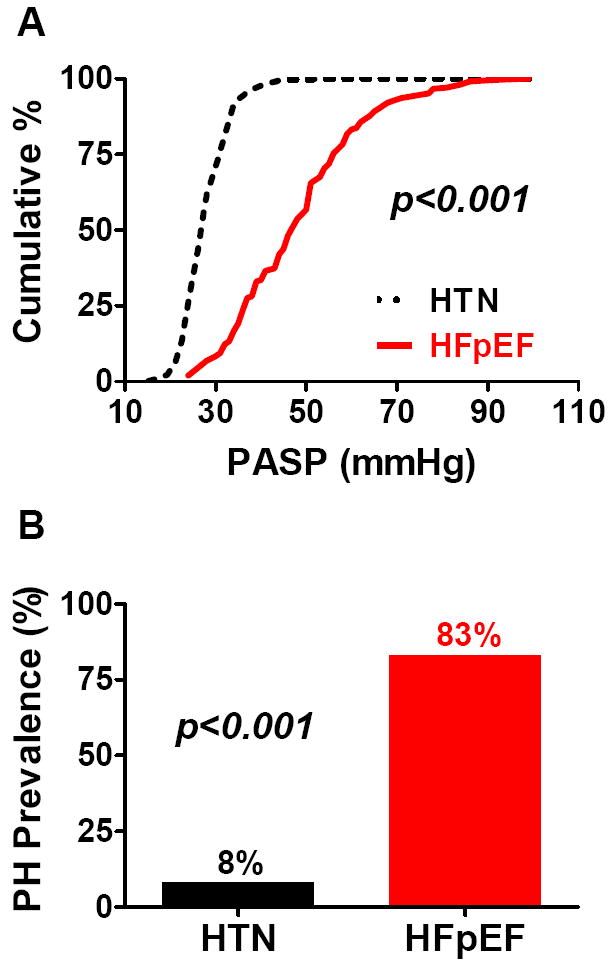
Methods: This community-based study of 244 HFpEF patients (age 76 +/- 13 years; 45% male) was followed up using Doppler echocardiography over 3 years. Control subjects were 719 adults with HTN without HF (age 66 +/- 10 years; 44% male). Pulmonary artery systolic pressure (PASP) was derived from the tricuspid regurgitation velocity and PH defined as PASP >35 mm Hg. Pulmonary capillary wedge pressure (PCWP) was estimated from the ratio of early transmitral flow velocity to early mitral annular diastolic velocity.
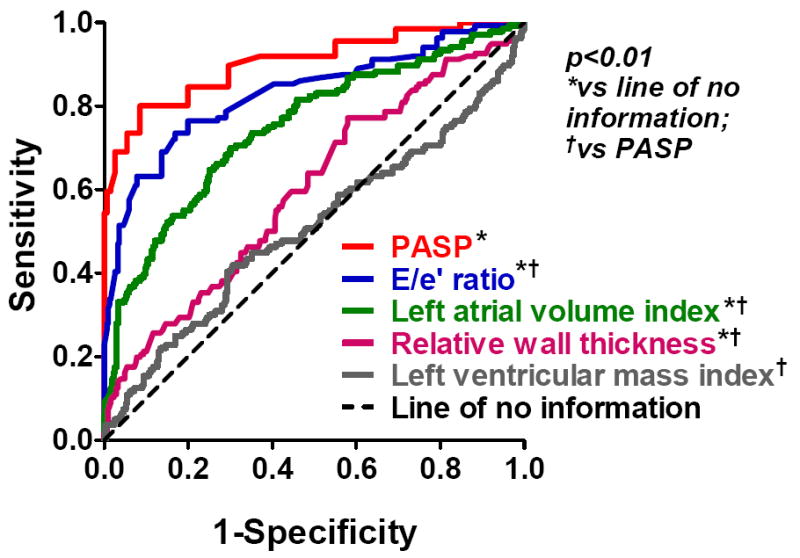
Results: In HFpEF, PH was present in 83% and the median (25th, 75th percentile) PASP was 48 (37, 56) mm Hg. PASP increased with PCWP (r = 0.21; p < 0.007). Adjusting for PCWP, PASP was higher in HFpEF than HTN (p < 0.001). The PASP distinguished HFpEF from HTN with an area under the receiver-operating characteristic curve of 0.91 (p < 0.001) and strongly predicted mortality in HFpEF (hazard ratio: 1.3 per 10 mm Hg; p < 0.001).
Conclusions: PH is highly prevalent and often severe in HFpEF. Although pulmonary venous HTN contributes to PH, it does not fully account for the severity of PH in HFpEF, suggesting that a component of pulmonary arterial HTN also contributes. The potent effect of PASP on mortality lends support for therapies aimed at pulmonary arterial HTN in HFpEF.
Figures


Comment in
-
The role of the pulmonary vasculature in heart failure with preserved ejection fraction.J Am Coll Cardiol. 2009 Mar 31;53(13):1127-9. doi: 10.1016/j.jacc.2009.01.006. J Am Coll Cardiol. 2009. PMID: 19324257 No abstract available.
-
Pulmonary hypertension in heart failure with preserved ejection fraction any pathophysiological role of mitral regurgitation.J Am Coll Cardiol. 2009 Sep 22;54(13):1191-2; author reply 1192. doi: 10.1016/j.jacc.2009.04.088. J Am Coll Cardiol. 2009. PMID: 19761945 No abstract available.
References
-
- Thompson W, White PD. Commonest Cause of Hypertrophy of the Right Ventricle-Left Ventricular Strain and Failure. Am Heart J. 1936;12:641–649.
-
- Abramson SV, Burke JF, Kelly JJ, Jr, et al. Pulmonary hypertension predicts mortality and morbidity in patients with dilated cardiomyopathy. Ann Intern Med. 1992;116:888–95. - PubMed
-
- Kessler KM, Willens HJ, Mallon SM. Diastolic left ventricular dysfunction leading to severe reversible pulmonary hypertension. Am Heart J. 1993;126:234–5. - PubMed
-
- Willens HJ, Kessler KM. Severe pulmonary hypertension associated with diastolic left ventricular dysfunction. Chest. 1993;103:1877–83. - PubMed
-
- Klapholz M, Maurer M, Lowe AM, et al. Hospitalization for heart failure in the presence of a normal left ventricular ejection fraction: results of the New York Heart Failure Registry. J Am Coll Cardiol. 2004;43:1432–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
