

Delayed-enhanced magnetic resonance imaging in nonischemic cardiomyopathy: utility for identifying the ventricular arrhythmia substrate
- PMID: 19324259
- PMCID: PMC2747602
- DOI: 10.1016/j.jacc.2008.11.052
Delayed-enhanced magnetic resonance imaging in nonischemic cardiomyopathy: utility for identifying the ventricular arrhythmia substrate
Abstract
Objectives: The purpose of this study was to assess the value of delayed-enhanced magnetic resonance imaging (DE-MRI) to guide ablation of ventricular arrhythmias in patients with nonischemic cardiomyopathy (NIC).
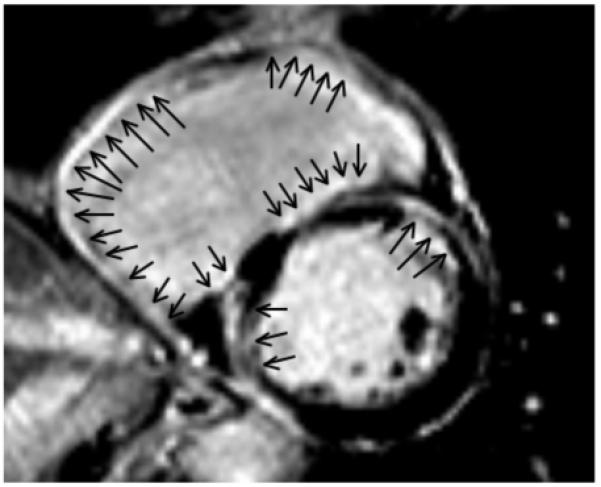
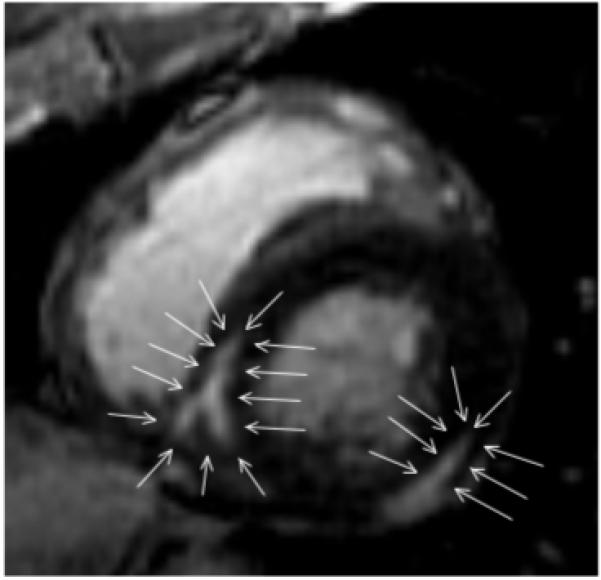
Background: In patients with NIC, ventricular arrhythmias often are associated with scar tissue. DE-MRI can be used to precisely define scar tissue.
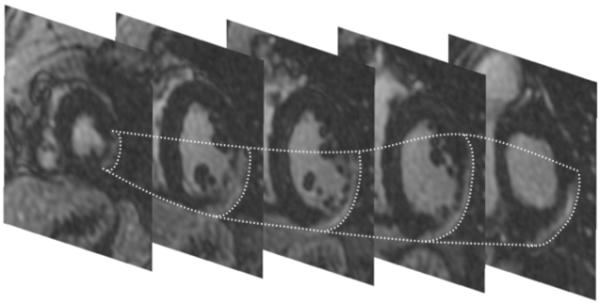
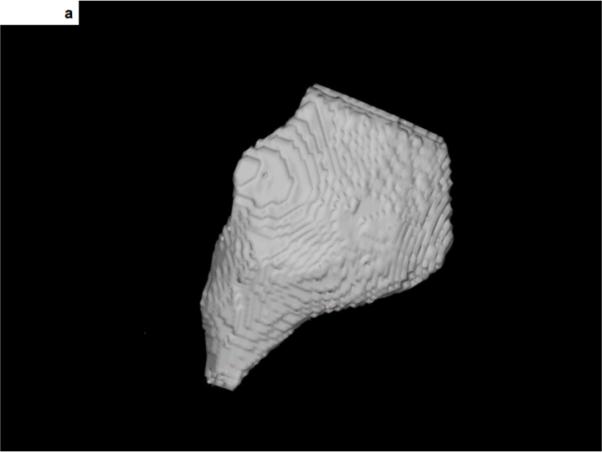
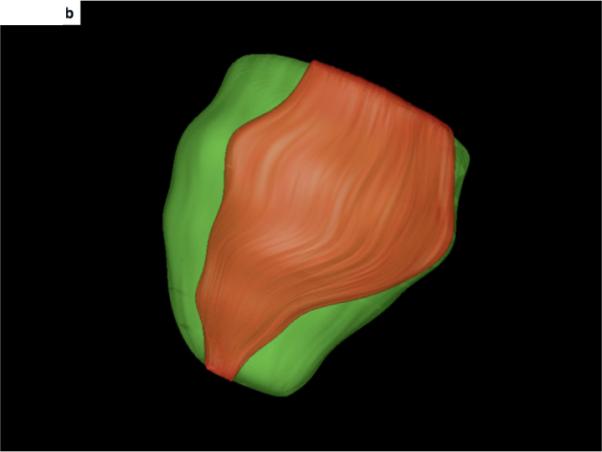
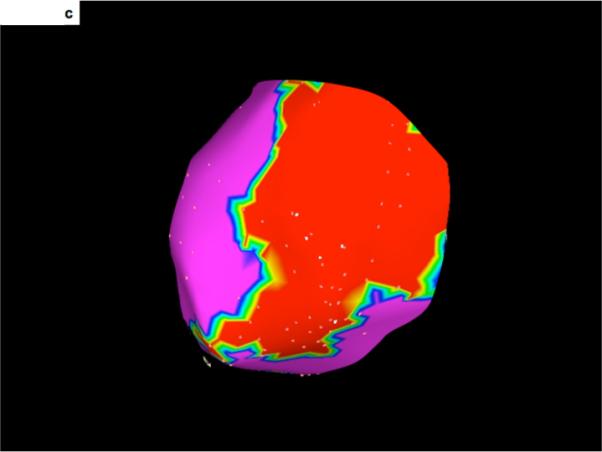
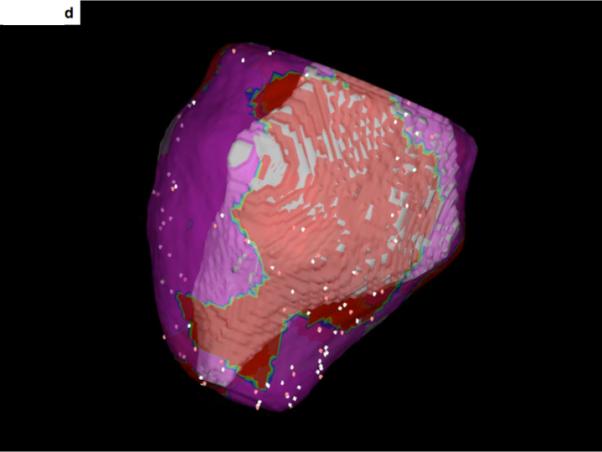
Methods: DE-MRI was performed in 29 consecutive patients (mean age 50 +/- 15 years) with NIC (mean ejection fraction 37 +/- 9%) referred for catheter ablation of ventricular tachycardia (VT) or premature ventricular complexes (PVCs). Scar was extracted from DE-MRIs and was then integrated into the electroanatomic map. Mapping data were correlated with respect to the localization of scar tissue.
Results: Scar was identified by DE-MRI in 14 of 29 patients. Nine of these patients had VT and 5 had PVCs. In 5 of the patients there was predominantly endocardial scar, and mapping and ablation of arrhythmias was effectively performed from the endocardium in all 5 patients. In 2 patients scar was either intramural or epicardial with extension to the endocardium. In both patients with partial endocardial scar extension, the ablation was effective in eliminating some but not all arrhythmias. In 2 patients most of the scar tissue was confined to the epicardium; mapping identified and eliminated an epicardial origin in both patients. No effect on arrhythmias could be achieved in the other 5 patients with predominantly intramural scar.
Conclusions: DE-MRI in patients without prior infarctions can help to identify the arrhythmogenic substrate; furthermore, it helps to plan an appropriate mapping and ablation strategy.
Figures
Comment in
-
Connecting the dots: the relevance of scar in nonischemic cardiomyopathy.J Am Coll Cardiol. 2009 Mar 31;53(13):1146-7. doi: 10.1016/j.jacc.2008.12.027. J Am Coll Cardiol. 2009. PMID: 19324260 Free PMC article. No abstract available.
References
-
- Nazarian S, Bluemke DA, Lardo AC, Zviman MM, Watkins SP, Dickfeld TL, Meininger GR, Roguin A, Calkins H, Tomaselli GF, Weiss RG, Berger RD, Lima JA, Halperin HR. Magnetic resonance assessment of the substrate for inducible ventricular tachycardia in nonischemic cardiomyopathy. Circulation. 2005;112:2821–5. - PMC - PubMed
-
- Assomull RG, Prasad SK, Lyne J, Smith G, Burman ED, Khan M, Sheppard MN, Poole-Wilson PA, Pennell DJ. Cardiovascular magnetic resonance, fibrosis, and prognosis in dilated cardiomyopathy. J Am Coll Cardiol. 2006;48:1977–85. - PubMed
-
- Wu KC, Weiss RG, Thiemann DR, Kitagawa K, Schmidt A, Dalal D, Lai S, Bluemke DA, Gerstenblith G, Marban E, Tomaselli GF, Lima JA. Late gadolinium enhancement by cardiovascular magnetic resonance heralds an adverse prognosis in nonischemic cardiomyopathy. J Am Coll Cardiol. 2008;51:2414–21. - PMC - PubMed
-
- McCrohon JA, Moon JC, Prasad SK, McKenna WJ, Lorenz CH, Coats AJ, Pennell DJ. Differentiation of heart failure related to dilated cardiomyopathy and coronary artery disease using gadolinium-enhanced cardiovascular magnetic resonance. Circulation. 2003;108:54–9. - PubMed
-
- De Cobelli F, Pieroni M, Esposito A, Chimenti C, Belloni E, Mellone R, Canu T, Perseghin G, Gaudio C, Maseri A, Frustaci A, Del Maschio A. Delayed gadolinium-enhanced cardiac magnetic resonance in patients with chronic myocarditis presenting with heart failure or recurrent arrhythmias. J Am Coll Cardiol. 2006;47:1649–54. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
