

Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock: 2007 update from the American College of Critical Care Medicine
- PMID: 19325359
- PMCID: PMC4447433
- DOI: 10.1097/CCM.0b013e31819323c6
Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock: 2007 update from the American College of Critical Care Medicine
Erratum in
- Crit Care Med. 2009 Apr;37(4):1536. Skache, Sara [corrected to Kache, Saraswati]; Irazusta, Jose [corrected to Irazuzta, Jose]
Abstract
Background: The Institute of Medicine calls for the use of clinical guidelines and practice parameters to promote "best practices" and to improve patient outcomes.
Objective: 2007 update of the 2002 American College of Critical Care Medicine Clinical Guidelines for Hemodynamic Support of Neonates and Children with Septic Shock.
Participants: Society of Critical Care Medicine members with special interest in neonatal and pediatric septic shock were identified from general solicitation at the Society of Critical Care Medicine Educational and Scientific Symposia (2001-2006).
Methods: The Pubmed/MEDLINE literature database (1966-2006) was searched using the keywords and phrases: sepsis, septicemia, septic shock, endotoxemia, persistent pulmonary hypertension, nitric oxide, extracorporeal membrane oxygenation (ECMO), and American College of Critical Care Medicine guidelines. Best practice centers that reported best outcomes were identified and their practices examined as models of care. Using a modified Delphi method, 30 experts graded new literature. Over 30 additional experts then reviewed the updated recommendations. The document was subsequently modified until there was greater than 90% expert consensus.
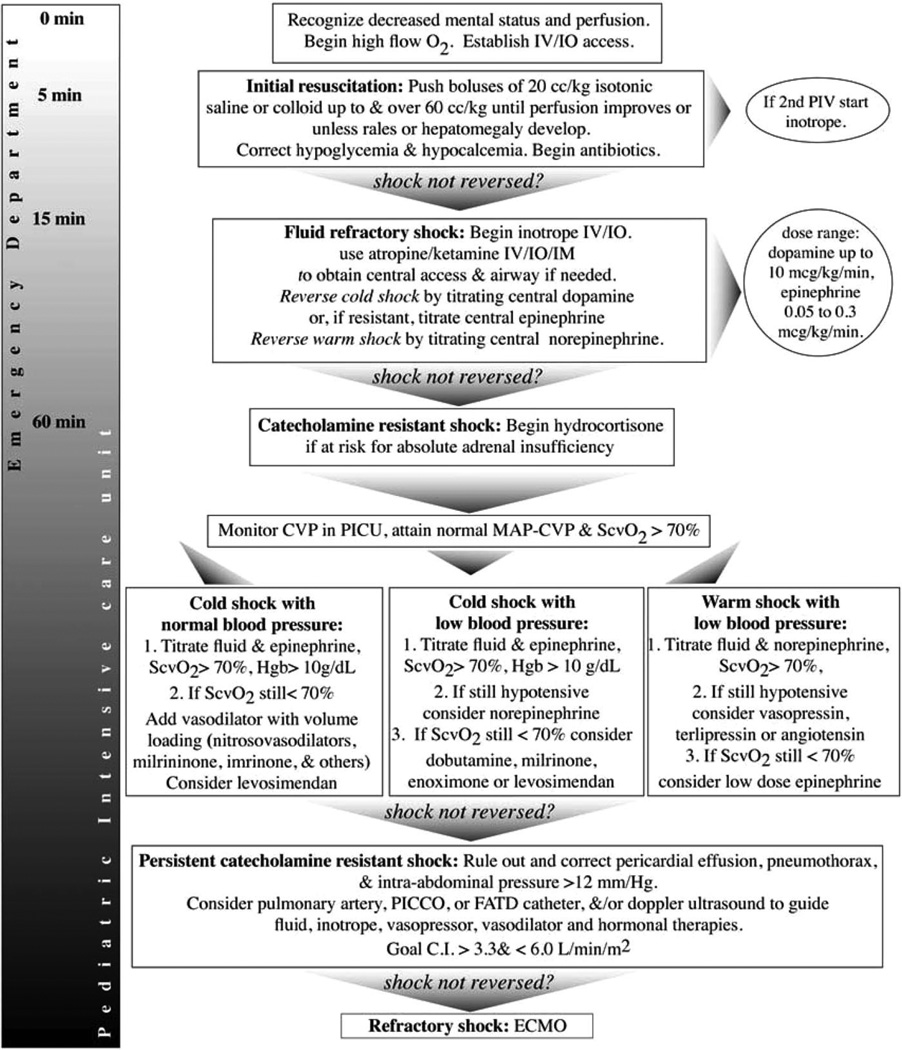
Results: The 2002 guidelines were widely disseminated, translated into Spanish and Portuguese, and incorporated into Society of Critical Care Medicine and AHA sanctioned recommendations. Centers that implemented the 2002 guidelines reported best practice outcomes (hospital mortality 1%-3% in previously healthy, and 7%-10% in chronically ill children). Early use of 2002 guidelines was associated with improved outcome in the community hospital emergency department (number needed to treat = 3.3) and tertiary pediatric intensive care setting (number needed to treat = 3.6); every hour that went by without guideline adherence was associated with a 1.4-fold increased mortality risk. The updated 2007 guidelines continue to recognize an increased likelihood that children with septic shock, compared with adults, require 1) proportionally larger quantities of fluid, 2) inotrope and vasodilator therapies, 3) hydrocortisone for absolute adrenal insufficiency, and 4) ECMO for refractory shock. The major new recommendation in the 2007 update is earlier use of inotrope support through peripheral access until central access is attained.
Conclusion: The 2007 update continues to emphasize early use of age-specific therapies to attain time-sensitive goals, specifically recommending 1) first hour fluid resuscitation and inotrope therapy directed to goals of threshold heart rates, normal blood pressure, and capillary refill <or=2 secs, and 2) subsequent intensive care unit hemodynamic support directed to goals of central venous oxygen saturation >70% and cardiac index 3.3-6.0 L/min/m.
Conflict of interest statement
The remaining authors have not disclosed any potential conflicts of interest.
Figures

Comment in
-
Pediatric sepsis: time is of the essence.Crit Care Med. 2009 Feb;37(2):785-6. doi: 10.1097/CCM.0b013e3181931210. Crit Care Med. 2009. PMID: 19325390 No abstract available.
-
Pediatric septic shock guidelines and extracorporeal membrane oxygenation management.Crit Care Med. 2009 Jun;37(6):2143-4; author reply 2144-5. doi: 10.1097/CCM.0b013e3181a5c33c. Crit Care Med. 2009. PMID: 19448486 No abstract available.
-
Norepinephrine in fluid-refractory catecholamine-resistant cold shock: are we sure?Crit Care Med. 2009 Jul;37(7):2322-3; author reply 2323. doi: 10.1097/CCM.0b013e3181a9f84c. Crit Care Med. 2009. PMID: 19535935 No abstract available.
-
Comment on the 2007 American College of Critical Care Medicine clinical guidelines for management of pediatric and neonatal septic shock.Crit Care Med. 2009 Jul;37(7):2324-5; author reply 2325. doi: 10.1097/CCM.0b013e3181aabc7c. Crit Care Med. 2009. PMID: 19535939 No abstract available.
-
Pediatric septic shock: let's talk about blood pressure.Crit Care Med. 2009 Dec;37(12):3190; author reply 3190-1. doi: 10.1097/CCM.0b013e3181bcb445. Crit Care Med. 2009. PMID: 19923954 No abstract available.
-
Epinephrine in pediatric septic shock: does the algorithm speak what the recommendations say?Crit Care Med. 2010 Apr;38(4):1237-8; author reply 1238. doi: 10.1097/CCM.0b013e3181d3ad7c. Crit Care Med. 2010. PMID: 20335731 No abstract available.
References
-
- DuPont HL, Spink WW. Infections due to gram negative organisms: An analysis of 860 patients with bacteremia at University of Minnesota Medical Center. 1958–1966. Medicine. 1969;48:307–332. - PubMed
-
- Stoll BJ, Holman RC, Shuchat A. Decline in sepsis-associated neonatal and infant deaths 1974–1994. Pediatrics. 1998;102:e18. - PubMed
-
- Angus DC, Linde Zwirble WT, Liddicker J, et al. Epidemiology of severe sepsis in the U.S.: Analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–1310. - PubMed
-
- Watson RS, Carcillo JA, Linde-Zwirble WT, et al. The epidemiology of severe sepsis in the United States. Am J Respir Crit Care Med. 2003;167:695–701. - PubMed
-
- Carcillo JA, Fields AI. American College of Critical Care Medicine Task Force Committee Members: Clinical practice parameters for hemodynamic support of pediatric and neonatal patients in septic shock. Crit Care Med. 2002;30:1365–1378. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
