

The Sequential Organ Failure Assessment score for predicting outcome in patients with severe sepsis and evidence of hypoperfusion at the time of emergency department presentation
- PMID: 19325482
- PMCID: PMC2703722
- DOI: 10.1097/CCM.0b013e31819def97
The Sequential Organ Failure Assessment score for predicting outcome in patients with severe sepsis and evidence of hypoperfusion at the time of emergency department presentation
Abstract
Objectives: Organ failure worsens outcome in sepsis. The Sequential Organ Failure Assessment (SOFA) score numerically quantifies the number and severity of failed organs. We examined the utility of the SOFA score for assessing outcome of patients with severe sepsis with evidence of hypoperfusion at the time of emergency department (ED) presentation.
Design: Prospective observational study.
Setting: Urban, tertiary ED with an annual census of >110,000.
Patients: ED patients with severe sepsis with evidence of hypoperfusion.
Inclusion criteria: suspected infection, two or more criteria of systemic inflammation, and either systolic blood pressure <90 mm Hg after a fluid bolus or lactate >or=4 mmol/L.
Exclusion criteria: age <18 years or need for immediate surgery.
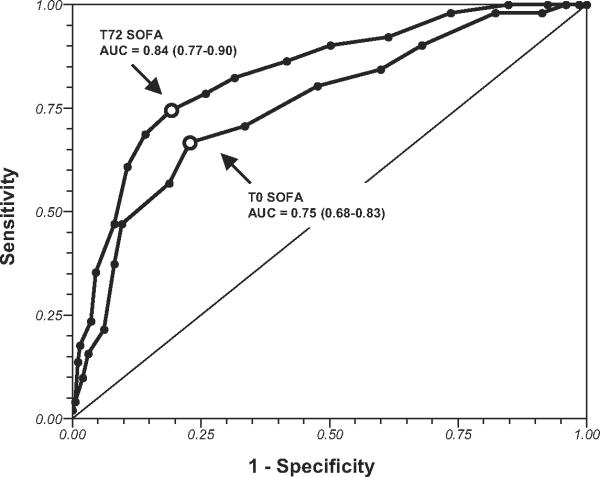
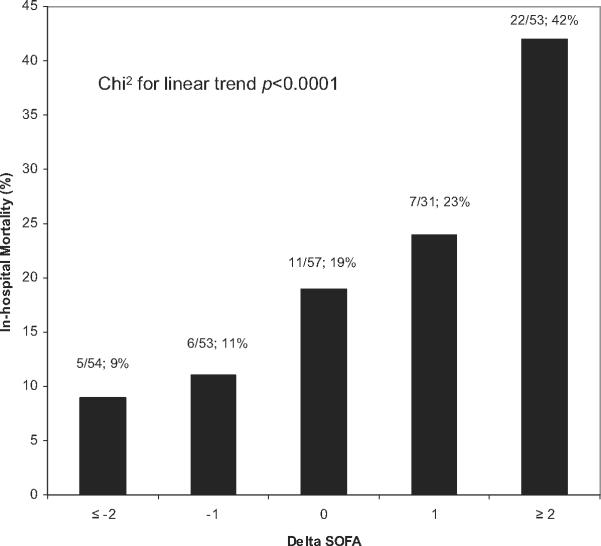
Interventions: SOFA scores were calculated at ED recognition (T0) and 72 hours after intensive care unit admission (T72). The primary outcome was in-hospital mortality. The area under the receiver operating characteristic curve was used to evaluate the predictive ability of SOFA scores at each time point. The relationship between Delta SOFA (change in SOFA from T0 to T72) was examined for linearity.
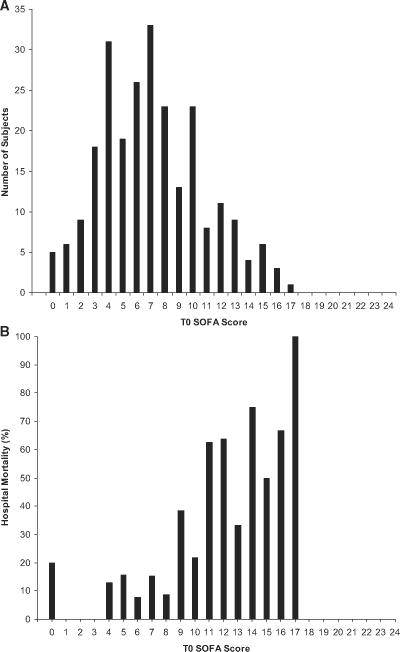
Results: A total of 248 subjects aged 57 +/- 16 years, 48% men, were enrolled over 2 years. All patients were treated with a standardized quantitative resuscitation protocol; the in-hospital mortality rate was 21%. The mean SOFA score at T0 was 7.1 +/- 3.6 points and at T72 was 7.4 +/- 4.9 points. The area under the receiver operating characteristic curve of SOFA for predicting in-hospital mortality at T0 was 0.75 (95% confidence interval 0.68-0.83) and at T72 was 0.84 (95% confidence interval 0.77-0.90). The Delta SOFA was found to have a positive relationship with in-hospital mortality.
Conclusions: The SOFA score provides potentially valuable prognostic information on in-hospital survival when applied to patients with severe sepsis with evidence of hypoperfusion at the time of ED presentation.
Figures
Comment in
-
Predictive models: the angel is in the details.Crit Care Med. 2009 May;37(5):1807-8. doi: 10.1097/CCM.0b013e3181a093cb. Crit Care Med. 2009. PMID: 19373053 No abstract available.
References
-
- Dombrovskiy VY, Martin AA, Sunderram J, et al. Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: A trend analysis from 1993 to 2003. Crit Care Med. 2007;35:1244–1250. - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–1310. - PubMed
-
- Strehlow MC, Emond SD, Shapiro NI, et al. National study of emergency department visits for sepsis, 1992 to 2001. Ann Emerg Med. 2006;48:326–331. - PubMed
-
- Fromm RJ, Gibbs LR, McCallum WG, et al. Critical care in the emergency department: A time-based study. Crit Care Med. 1993;21:970–976. - PubMed
-
- Wang HE, Shapiro NI, Angus DC, et al. National estimates of severe sepsis in United States emergency departments. Crit Care Med. 2007;35:1928–1936. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
