

Benefit of antiretroviral therapy on survival of human immunodeficiency virus-infected patients admitted to an intensive care unit
- PMID: 19325488
- PMCID: PMC4143892
- DOI: 10.1097/CCM.0b013e31819da8c7
Benefit of antiretroviral therapy on survival of human immunodeficiency virus-infected patients admitted to an intensive care unit
Abstract
Objective: To evaluate the impact of antiretroviral therapy (ART) and the prognostic factors for in-intensive care unit (ICU) and 6-month mortality in human immunodeficiency virus (HIV)-infected patients.
Design: A retrospective cohort study was conducted in patients admitted to the ICU from 1996 through 2006. The follow-up period extended for 6 months after ICU admission.
Setting: The ICU of a tertiary-care teaching hospital at the Universidade de São Paulo, Brazil.
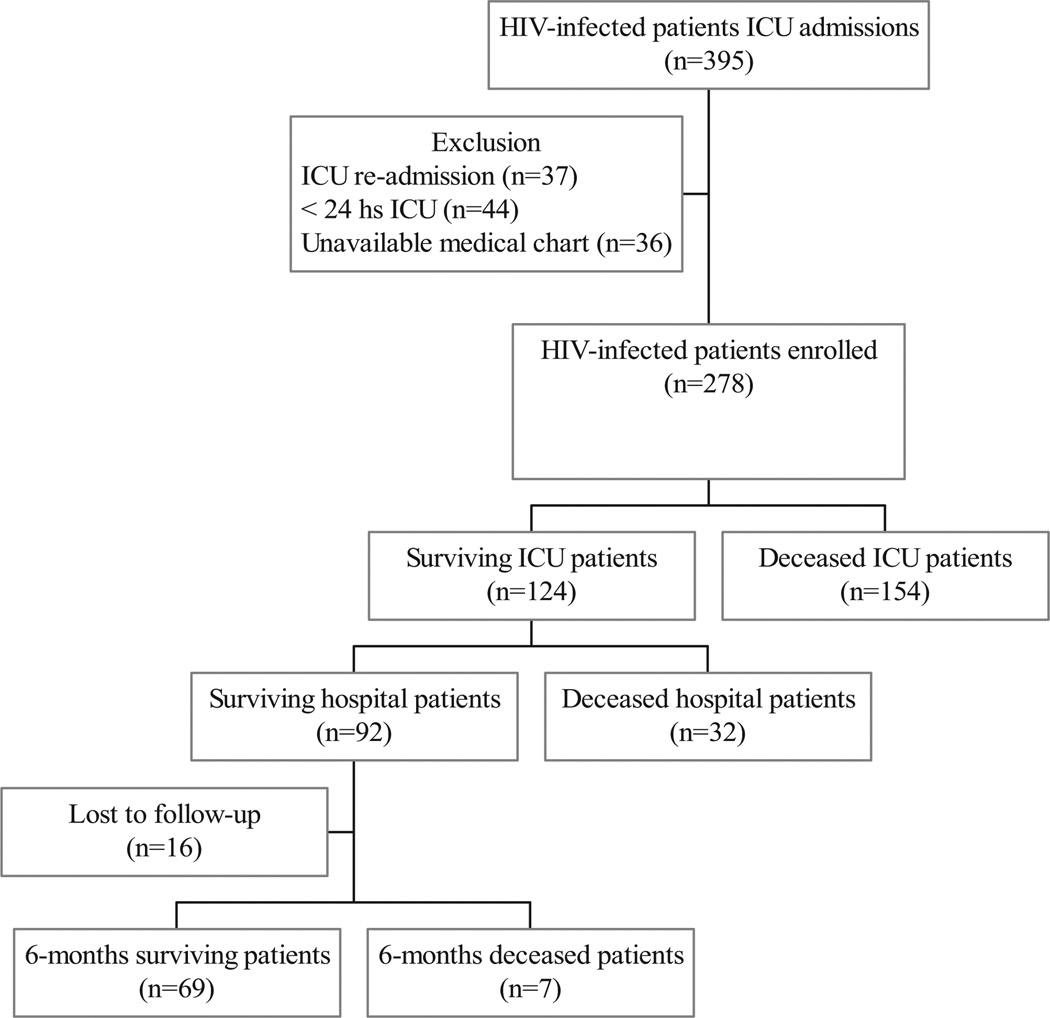
Participants: A total of 278 HIV-infected patients admitted to the ICU were selected. We excluded ICU readmissions (37), ICU admissions who stayed less than 24 hours (44), and patients with unavailable medical charts (36).
Outcome measure: In-ICU and 6-month mortality.
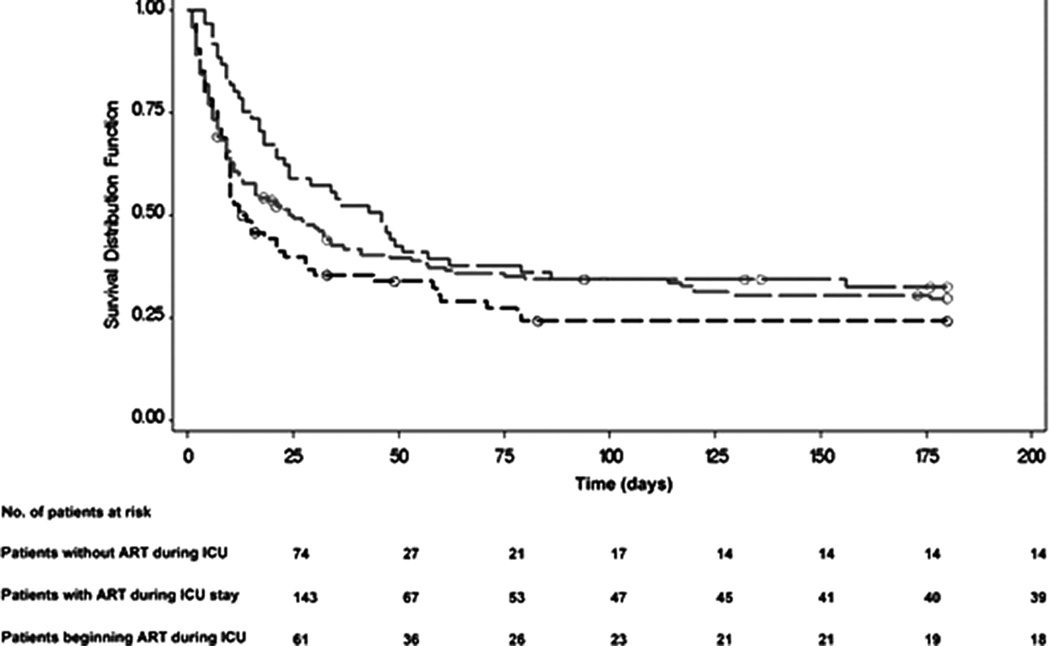
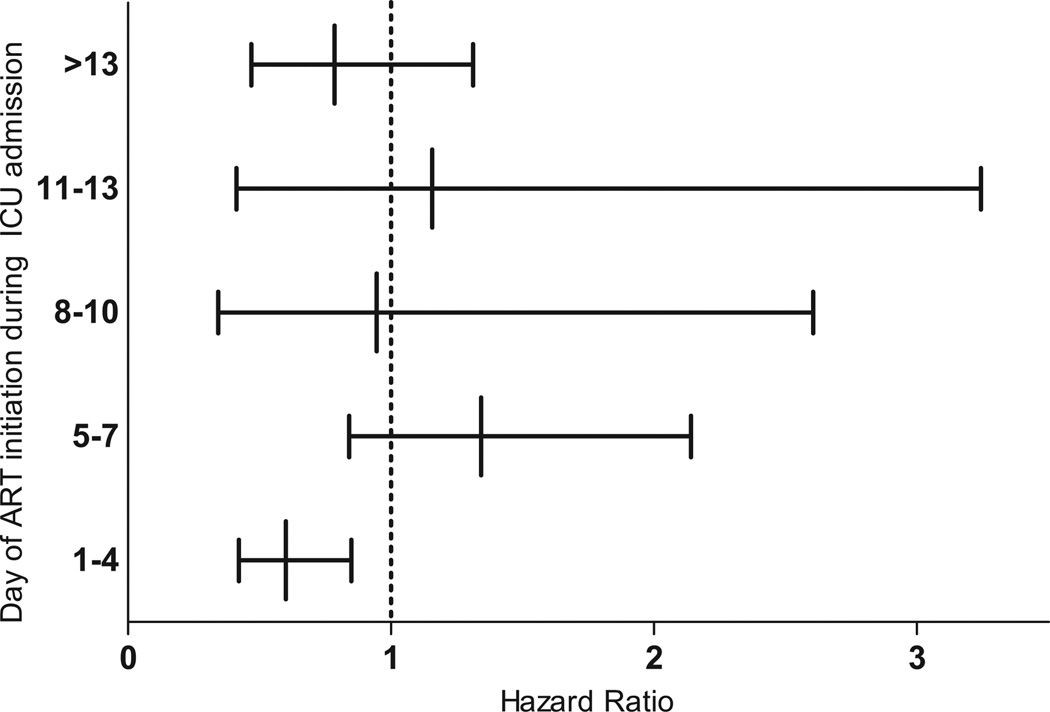
Main results: Multivariate logistic regression analysis and Cox proportional hazards models demonstrated that the variables associated with in-ICU and 6-month mortality were sepsis as the cause of admission (odds ratio [OR] = 3.16 [95% confidence interval [CI] 1.65-6.06]); hazards ratio [HR] = 1.37 [95% CI 1.01-1.88]), an Acute Physiology and Chronic Health Evaluation II score >19 [OR = 2.81 (95% CI 1.57-5.04); HR = 2.18 (95% CI 1.62-2.94)], mechanical ventilation during the first 24 hours [OR = 3.92 (95% CI 2.20-6.96); HR = 2.25 (95% CI 1.65-3.07)], and year of ICU admission [OR = 0.90 (95% CI 0.81-0.99); HR = 0.92 [95% CI 0.87-0.97)]. CD4 T-cell count <50 cells/mm(3) was only associated with ICU mortality [OR = 2.10 (95% CI 1.17-3.76)]. The use of ART in the ICU was negatively predictive of 6-month mortality in the Cox model [HR = 0.50 (95% CI 0.35-0.71)], especially if this therapy was introduced during the first 4 days of admission to the ICU [HR = 0.58 (95% CI 0.41-0.83)]. Regarding HIV-infected patients admitted to ICU without using ART, those who have started this treatment during ICU stay presented a better prognosis when time and potential confounding factors were adjusted for [HR 0.55 (95% CI 0.31-0.98)].
Conclusions: The ICU outcome of HIV-infected patients seems to be dependent not only on acute illness severity, but also on the administration of antiretroviral treatment.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Kaplan JE, Hanson D, Dworkin MS, et al. Epidemiology of human immunodeficiency virus-associated opportunistic infections in the United States in the era of highly active antiretroviral therapy. Clin Infect Dis. 2000;30(Suppl 1):S5–S14. - PubMed
-
- Moore RD, Chaisson RE. Natural history of HIV infection in the era of combination antiretroviral therapy. Aids. 1999;13:1933–1942. - PubMed
-
- Palella FJ, Jr, Delaney KM, Moorman AC, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998;338:853–860. - PubMed
-
- Moore RD, Chaisson RE. Natural history of opportunistic disease in an HIV-infected urban clinical cohort. Ann Intern Med. 1996;124:633–642. - PubMed
-
- Narasimhan M, Posner AJ, DePalo VA, et al. Intensive care in patients with HIV infection in the era of highly active antiretroviral therapy. Chest. 2004;125:1800–1804. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
