

Development, feasibility, and acceptability of the Family/Adolescent-Centered (FACE) Advance Care Planning intervention for adolescents with HIV
- PMID: 19327074
- PMCID: PMC2991180
- DOI: 10.1089/jpm.2008.0261
Development, feasibility, and acceptability of the Family/Adolescent-Centered (FACE) Advance Care Planning intervention for adolescents with HIV
Abstract
Objectives: To develop, adapt, and ensure feasibility, acceptability, and safety of the Family/Adolescent-Centered (FACE) Advance Care Planning intervention.
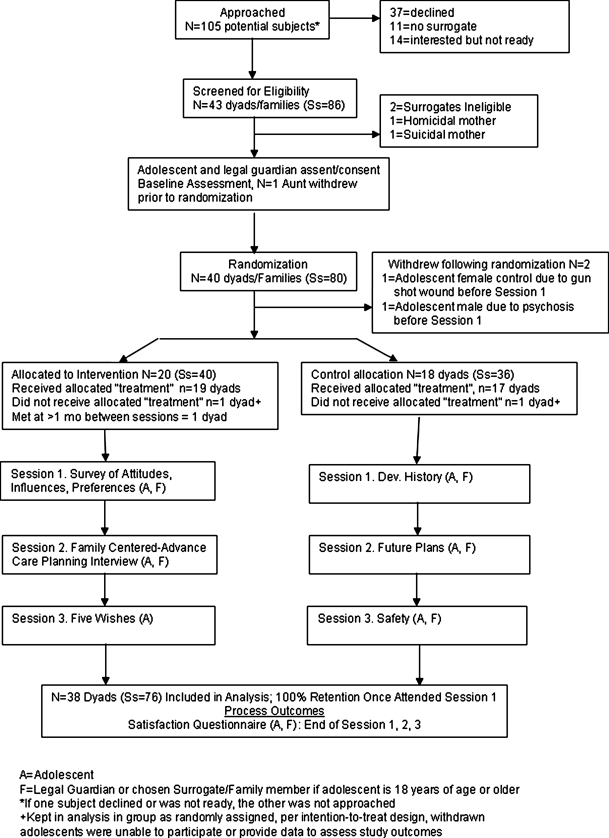
Patients and methods: Two-group, randomized, controlled trial in two hospital-based outpatient clinics in Washington, D.C. and Memphis, Tennessee, from 2006 to 2008 was conducted. Participants (n = 38 dyads) included medically stable adolescents aged 14 to 21 years with HIV/AIDS and surrogates/families over age 20. Three 60- to 90-minute sessions were conducted via a semistructured family interview with a trained/certified interviewer. Intervention received: (1) Lyon Advance Care Planning Survey; (2) Respecting Choices interview; and (3) Five Wishes. Control received (1) Developmental History, (2) Health Tips, and (3) Future Plans. Feasibility was measured by percent enrollment, attendance, retention, and completeness of data. Acceptability and safety were measured by Satisfaction Questionnaire, using longitudinal regression analysis.
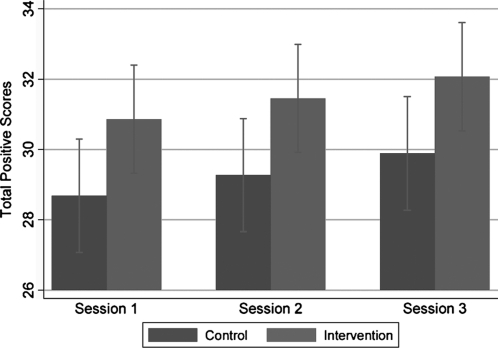
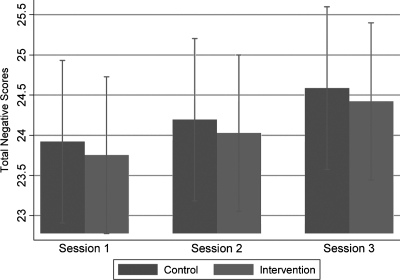
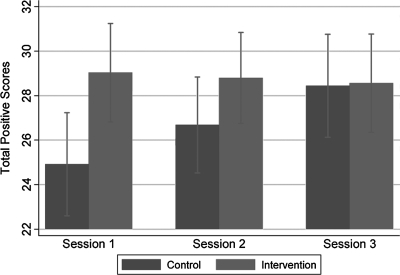
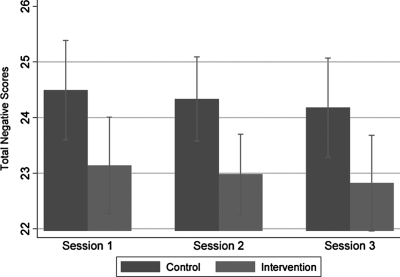
Results: Adolescents' mean age was 16 years; 40% were males; 92% were black; HIV transmission rate was 68% perinatal and 32% sexually acquired; 42% were asymptomatic; 29% were symptomatic; and 29% had a diagnosis of AIDS. Intervention adolescents were more likely to rate sessions positively (p = 0.002) and less likely to rate sessions negatively (p = 0.011) than controls. Guardians/surrogates were more likely to rate the sessions positively (p = 0.041) and demonstrated no difference in rating sessions negatively (p = 0.779) than controls.
Conclusions: Existing advance care planning models can be adapted for age, disease, and culture. Adolescents with HIV/AIDS were satisfied with an advance care planning approach that facilitated discussion about their end-of-life wishes with their families. Families acknowledged a life-threatening condition and were willing to initiate end-of-life conversations when their adolescents were medically stable.
Figures
References
-
- American Academy of Pediatrics. Committee on Bioethics and Committee on Hospital Care. Palliative care for children. Pediatrics. 2000;106:351–357. - PubMed
-
- Field MJ, editor; Behrman RE, editor. When Children Die: Improving Palliative and End-of-Life Care for Children and their Families. Washington, D.C.: Institute of Medicine, National Academy Press; 2002. - PubMed
-
- Hinds PS. Drew D. Oakes LL. Fouladi M. Spunt SL. Church C. Furman WL. End-of-life care preferences of pediatric patients with cancer. J Clin Oncol. 2005;23:9055–9057.
-
- Lyon ME. McCabe MA. Patel K. D'Angelo LJ. What do adolescents want? An exploratory study regarding end-of-life decision-making. http://journals.elsevierhealth.com/periodicals/jah. [Feb 11;2009 ];J Adolesc Health. 2004 35:529. - PubMed
-
- Walsh-Kelly CM. Lang KR. Chevako J. Blank EL. Korom N. Kirk K. Gray A. Advance directives in a pediatric emergency department. Pediatrics. 1999;103:826–830. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
