

Blood pressure reduction, persistence and costs in the evaluation of antihypertensive drug treatment--a review
- PMID: 19327149
- PMCID: PMC2669450
- DOI: 10.1186/1475-2840-8-18
Blood pressure reduction, persistence and costs in the evaluation of antihypertensive drug treatment--a review
Abstract
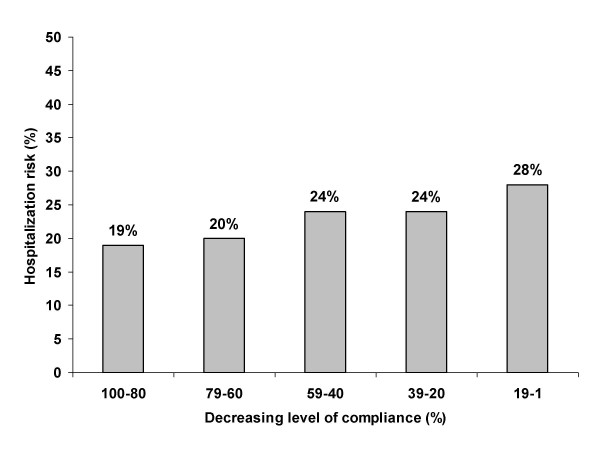
Background: Blood pressure lowering drugs are usually evaluated in short term trials determining the absolute blood pressure reduction during trough and the duration of the antihypertensive effect after single or multiple dosing. A lack of persistence with treatment has however been shown to be linked to a worse cardiovascular prognosis. This review explores the blood pressure reduction and persistence with treatment of antihypertensive drugs and the cost consequences of poor persistence with pharmaceutical interventions in arterial hypertension.
Methods: We have searched the literature for data on blood pressure lowering effects of different antihypertensive drug classes and agents, on persistence with treatment, and on related costs. Persistence was measured as patients' medication possession rate. Results are presented in the form of a systematic review.
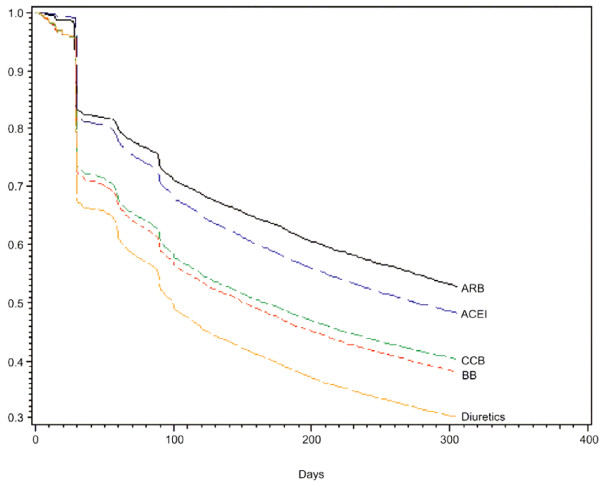
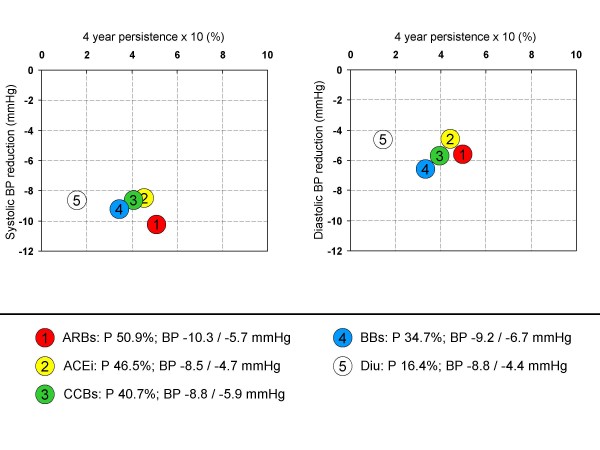
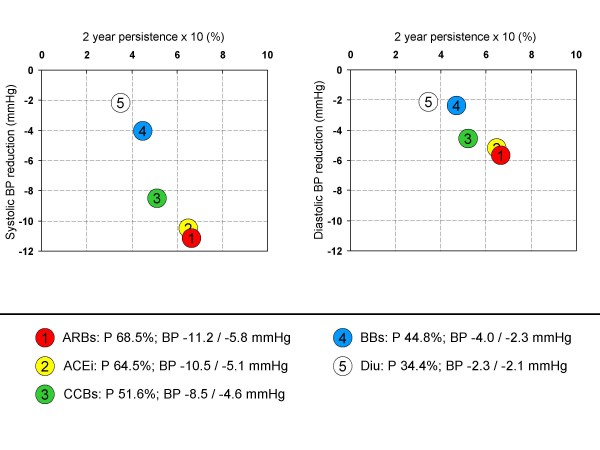
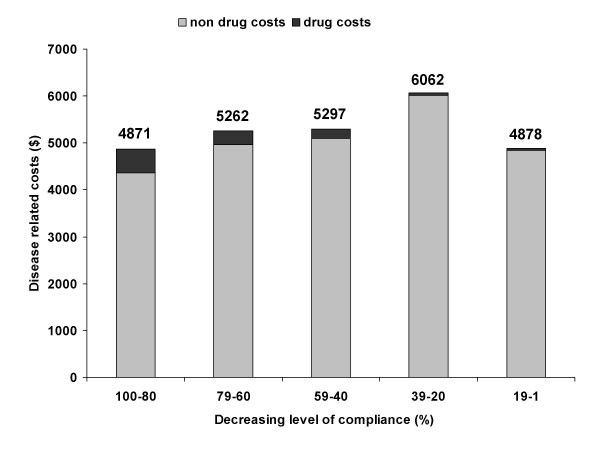
Results: Angiotensin II receptor blocker (ARBs) have a competitive blood pressure lowering efficacy compared with ACE-inhibitors (ACEi) and calcium channel blockers (CCBs), beta-blockers (BBs) and diuretics. 8 studies describing the persistence with treatment were identified. Patients were more persistent on ARBs than on ACEi and CCBs, BBs and diuretics. Thus the product of blood pressure lowering and persistence was higher on ARBs than on any other drug class. Although the price per tablet of more recently developed drugs (ACEi, ARBs) is higher than that of older ones (diuretics and BBs), the newer drugs result in a more favourable cost to effect ratio when direct drug costs and indirect costs are also considered.
Conclusion: To evaluate drugs for the treatment of hypertension several key variables including the blood pressure lowering effect, side effects, compliance/persistence with treatment, as well as drug costs and direct and indirect costs of medical care have to be considered. ARBs, while nominally more expensive when drug costs are considered only, provide substantial cost savings and may prevent cardiovascular morbidity and mortality based on the more complete antihypertensive coverage. This makes ARBs an attractive choice for long term treatment of hypertension.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
