

Positive end-expiratory pressure alters the severity and spatial heterogeneity of ventilator-induced lung injury: an argument for cyclical airway collapse
- PMID: 19327294
- PMCID: PMC2720092
- DOI: 10.1016/j.jcrc.2008.04.005
Positive end-expiratory pressure alters the severity and spatial heterogeneity of ventilator-induced lung injury: an argument for cyclical airway collapse
Abstract
Purpose: Ventilator-induced lung injury (VILI) is a recognized complication of mechanical ventilation. Although the specific mechanism by which mechanical ventilation causes lung injury remains an active area of study, both alveolar overdistension and cyclical airway collapse and recruitment have been suggested as contributing causes. We hypothesized that mechanical ventilation in the absence of positive end-expiratory pressure (PEEP) causes VILI to be more severe and regionally variable as compared with PEEP = 8 cm H(2)O.
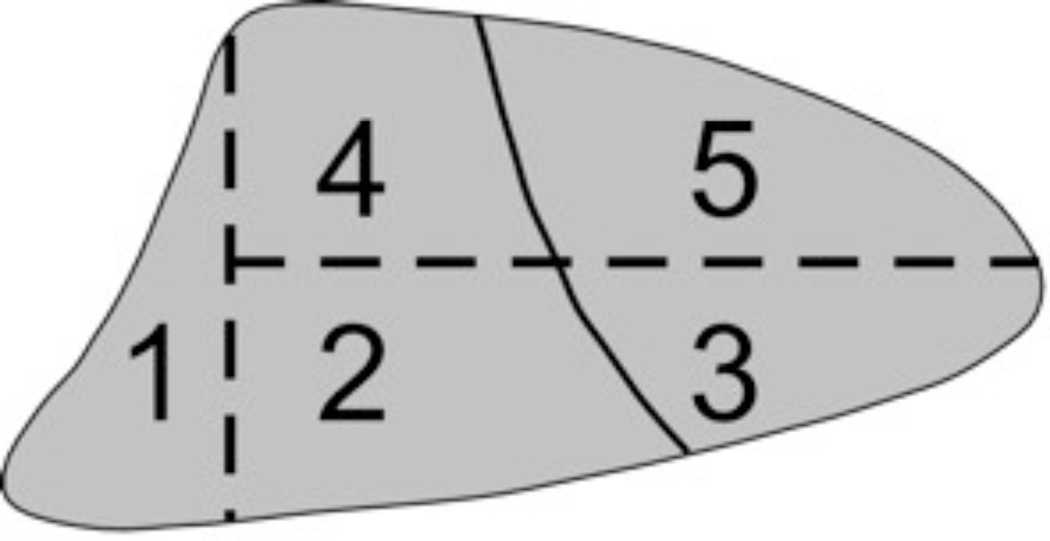
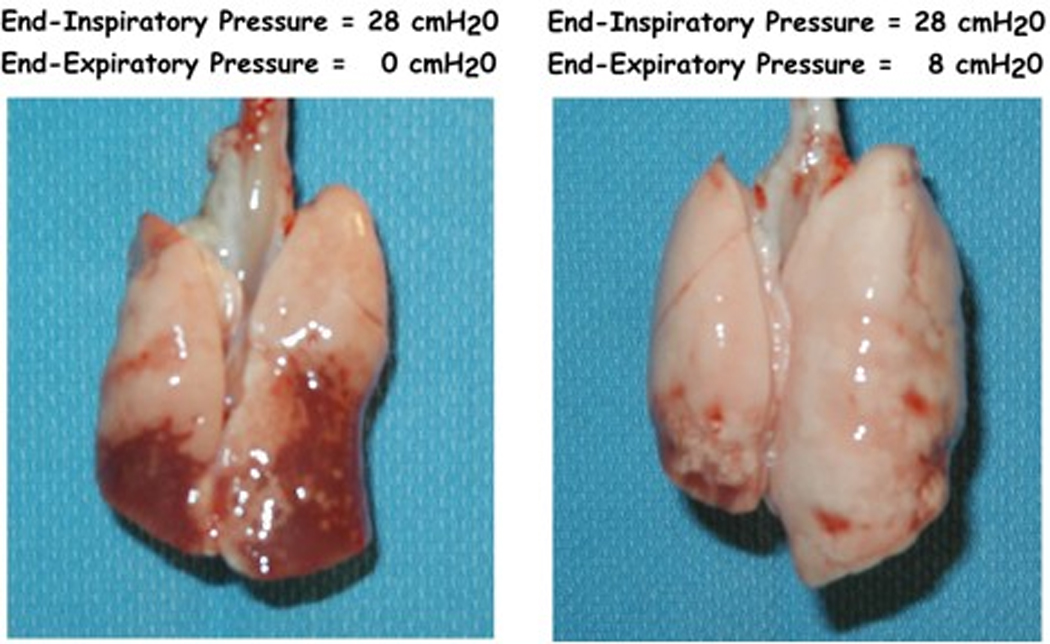
Materials and methods: To test this hypothesis, anesthetized, supine rabbits were mechanically ventilated with an end-inspiratory pressure of 28 cm H(2)O and either 0 or 8 cm H(2)O PEEP for 4 hours. Regional lung injury was determined by histologic scoring.
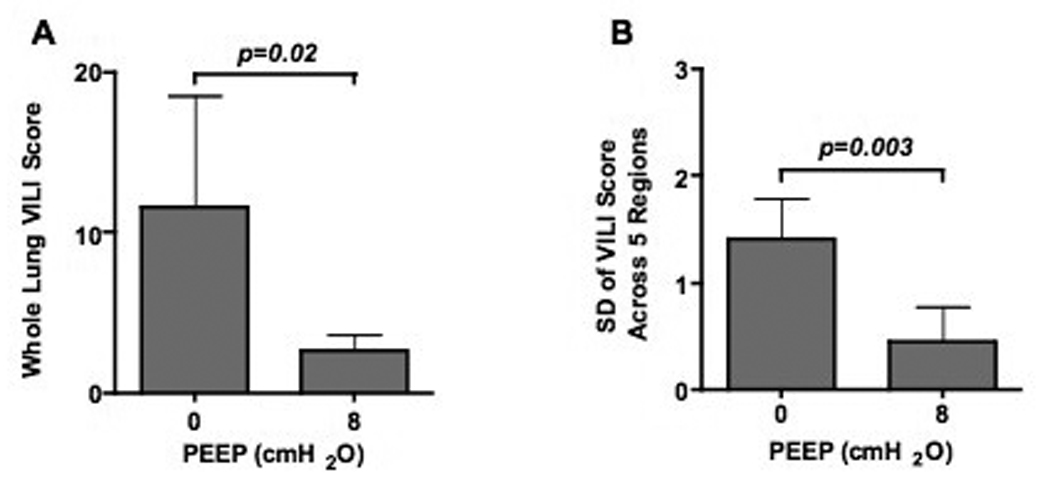
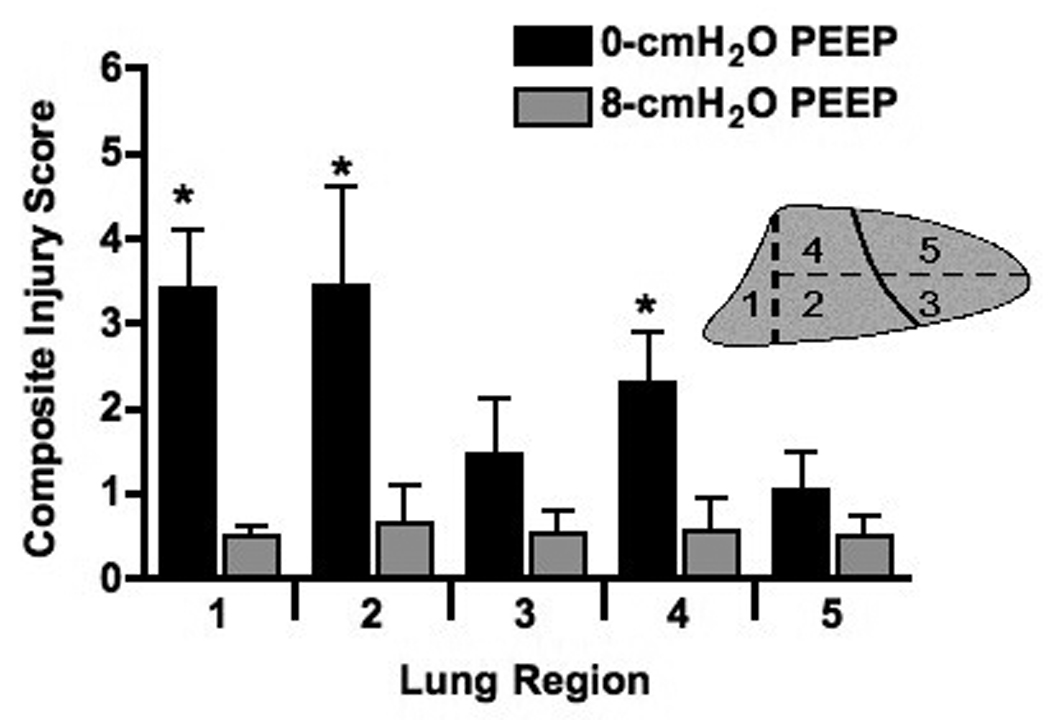
Results: In the absence of PEEP, lung injury was regionally variable and greatest in the dorsal-caudal lung. This regional injury heterogeneity was abolished by the addition of PEEP = 8 cm H(2)O.
Conclusions: These results suggest that VILI is regionally heterogeneous and spatially correlates with regions in which cyclical airway collapse and recruitment is most likely to occur.
Figures
References
-
- Dreyfuss D, Basset G, Soler P, et al. Intermittent positive-pressure hyperventilation with high inflation pressures produces pulmonary microvascular injury in rats. Am Rev Respir Dis. 1985;132(4):880–884. - PubMed
-
- Dreyfuss D, Soler P, Basset G, et al. High inflation pressure pulmonary edema. Respective effects of high airway pressure, high tidal volume, and positive end-expiratory pressure. Am Rev Respir Dis. 1988;137(5):1159–1164. - PubMed
-
- Webb HH, Tierney DF. Experimental pulmonary edema due to intermittent positive pressure ventilation with high inflation pressures. Protection by positive end-expiratory pressure. Am Rev Respir Dis. 1974;110(5):556–565. - PubMed
-
- Sinclair S, Souders J, Hlastala M. Severity and distribution of ventilator-induced lung injury is altered by PEEP, prone position, and respiratory frequency in normal rabbits. Am J Respir Crit Care Med. 1998;157(153):A107.
-
- Sinclair SE, Kregenow DA, Lamm WJ, et al. Hypercapnic acidosis is protective in an in vivo model of ventilator-induced lung injury. Am J Respir Crit Care Med. 2002;166(3):403–408. - PubMed
