

Congenital amegakaryocytic thrombocytopenia and thrombocytopenia with absent radii
- PMID: 19327586
- PMCID: PMC2757092
- DOI: 10.1016/j.hoc.2009.01.012
Congenital amegakaryocytic thrombocytopenia and thrombocytopenia with absent radii
Abstract
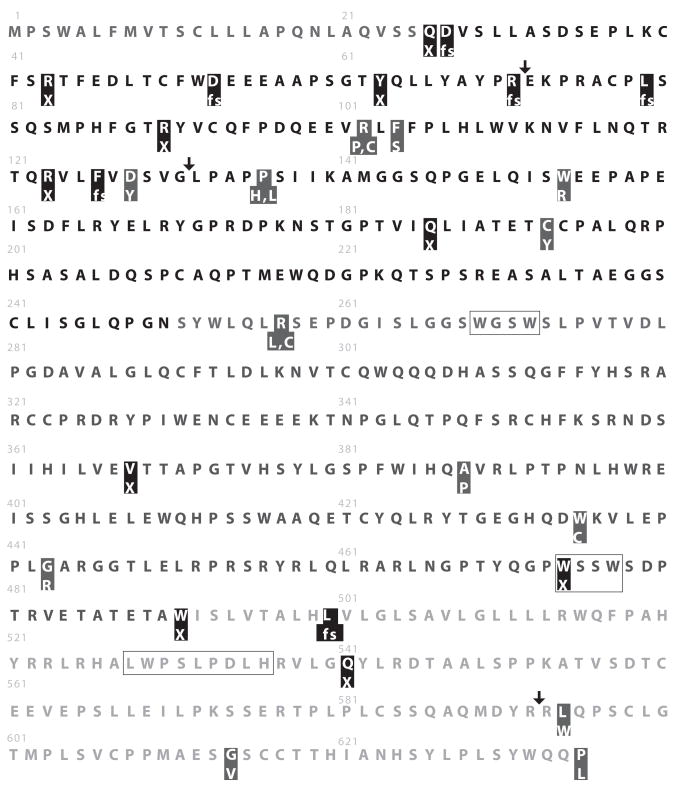
Thrombocytopenia is a relatively common clinical problem in hospitalized neonates, and it is critical to distinguish infants who have rare congenital thrombocytopenias from those who have acquired disorders. Two well-described inherited thrombocytopenia syndromes that present in the newborn period are congenital amegakaryocytic thrombocytopenia (CAMT) and thrombocytopenia with absent radii (TAR). Although both are characterized by severe (< 50,000/microL) thrombocytopenia at birth, the molecular mechanisms underlying these disorders and their clinical presentations and courses are distinct. CAMT is an autosomal recessive disorder caused by mutations in the thrombopoietin (TPO) receptor c-Mpl. TAR is a syndrome of variable inheritance and unclear genetic etiology consisting of thrombocytopenia in association with bilateral absent radii and frequently additional congenital abnormalities. This article summarizes the current understanding of the pathophysiology and clinical course of CAMT and TAR.
Figures
References
-
- King S, Germeshausen M, Strauss G, Welte K, et al. Congenital amegakaryocytic thrombocytopenia: a retrospective clinical analysis of 20 patients. Br J Haematol. 2005 Dec;131(5):636–644. - PubMed
-
- Rose MJ, Nicol KK, Skeens MA, Gross TG, et al. Congenital amegakaryocytic thrombocytopenia: The diagnostic importance of combining pathology with molecular genetics. Pediatr Blood Cancer. 2008 Jan 31; - PubMed
-
- Ballmaier M, Germeshausen M, Schulze H, et al. c-mpl mutations are the cause of congenital amegakaryocytic thrombocytopenia. Blood. 2001 Jan 1;97(1):139–146. - PubMed
-
- Germeshausen M, Ballmaier M, Welte K. MPL mutations in 23 patients suffering from congenital amegakaryocytic thrombocytopenia: the type of mutation predicts the course of the disease. Hum Mutat. 2006 Mar;27(3):296. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
