

[Prospective study to evaluate diagnostic accuracy in benign anal diseases in primary care]
- PMID: 19328596
- PMCID: PMC7665109
- DOI: 10.1016/j.aprim.2008.07.001
[Prospective study to evaluate diagnostic accuracy in benign anal diseases in primary care]
Abstract
Objective: To analyse the diagnostic performance of the primary care (PC) doctor in benign anal diseases.
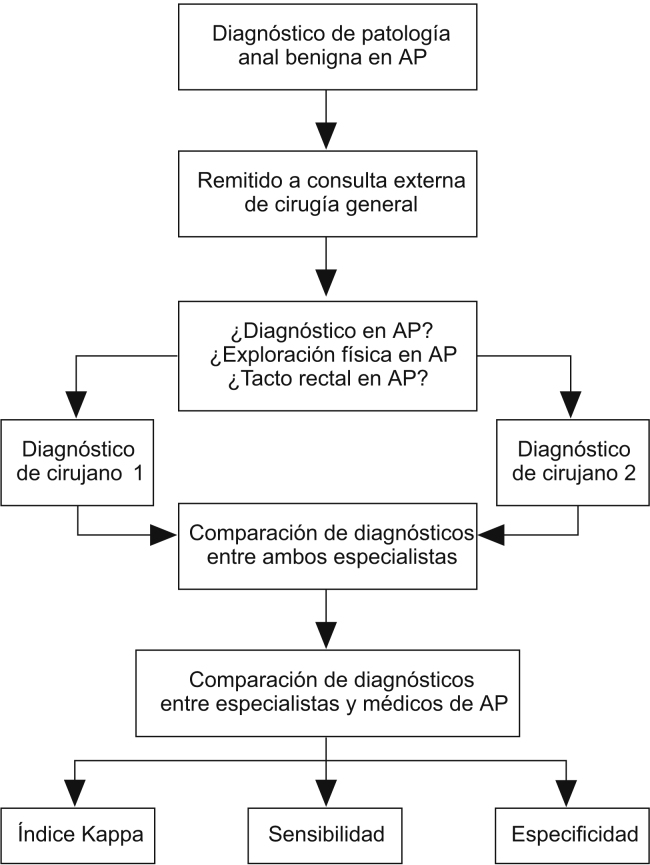
Design: Cross-sectional study including patients referred to our clinic from PC with the diagnosis of clinical conditions pertaining to benign anal diseases between 1st June and 31st December 2007. The diagnosis established by the PC doctor was compared with that of 2 medical specialists in general and digestive diseases surgery.
Setting: Department of General Surgery and Digestive Diseases. Castellon General Hospital.
Participants: Patients diagnosed with a benign anal disease in PC and referred to our department.
Measurements: The sensitivity, specificity and kappa index was calculated for each disease.
Results: A total of 105 patients were included. The diagnoses were: 65 haemorrhoids, 13 fissures, 8 fistulas, 7 abscesses, 4 pilonidal cysts, and 8 other diagnoses. A physical examination was carried out on 61 patients and 19 had a rectal examination. In AE, 44 haemorrhoids, 20 fissures, 9 pilonidal cysts were diagnosed and there were 16 other diagnoses. For haemorrhoids the sensitivity was 90.9%, the specificity 59%, and the kappa index was 0.5. For a fistula, it was 43.8%, 98.9% and 0.5, respectively and for a fissure, 15%, 88.2% and 0.04. The physical examination improved all these results.
Conclusions: The diagnostic performance of benign anal diseases in PC is insufficient. A good physical examination and improved training in these diseases could possibly improve these results.
Objetivo: Analizar el rendimiento diagnóstico del médico de atención primaria (AP) en enfermedad anal benigna.
Diseño: Estudio transversal con inclusión de los pacientes remitidos desde AP a nuestra consulta con el diagnóstico de entidades Clínicas englobadas en la enfermedad anal benigna entre el 1 de junio y el 31 de diciembre de 2007. Se comparó el diagnóstico establecido por el médico de AP con el de 2 médicos especialistas en cirugía general y digestiva.
Emplazamiento: Servicio de Cirugía General y del Aparato Digestivo. Hospital General de Castellón.
Participantes: Pacientes diagnosticados de enfermedad anal benigna en AP y remitidos a nuestro servicio.
Mediciones: Se calcularon, para cada enfermedad, la sensibilidad, la especificidad y los índices kappa.
Resultados: Se intervino en un total de 105 pacientes. Los diagnósticos en AP fueron: 65 hemorroides, 13 fisuras, 8 fístulas, 7 abscesos, 4 quistes pilonidales y 8 otros diagnósticos. A 61 pacientes se les había realizado exploración física y a 19, tacto rectal. En atención especializada se diagnosticaron 44 hemorroides, 20 fisuras, 16 fístulas, 9 quistes pilonidales y 16 otros diagnósticos. Para hemorroides, la sensibilidad fue del 90,9%, la especificidad del 59% y el índice kappa, 0,5. Para fístula, el 43,8%, el 98,9% y 0,5, respectivamente, y para fisura, el 15%, el 88,2% y 0,04. La exploración física mejoró todos estos resultados.
Conclusiones: El rendimiento diagnóstico de la enfermedad anal benigna en AP es insuficiente. Posiblemente, una buena exploración física y una mejor formación en estas enfermedades conseguirían mejorar estos resultados.
Figures
Comment in
-
[Diagnostic yield in benign anal disease in primary care].Aten Primaria. 2009 Oct;41(10):582-3; author reply 583. doi: 10.1016/j.aprim.2009.06.011. Epub 2009 Sep 9. Aten Primaria. 2009. PMID: 19740569 Free PMC article. Spanish. No abstract available.
Similar articles
-
Prospective analysis of clinician accuracy in the diagnosis of benign anal pathology: comparison across specialties and years of experience.Dis Colon Rectum. 2010 Jan;53(1):47-52. doi: 10.1007/DCR.0b013e3181bbfc89. Dis Colon Rectum. 2010. PMID: 20010350
-
[Daily aspects of proctology].Rev Med Brux. 1995 Jul-Aug;16(4):267-70. Rev Med Brux. 1995. PMID: 7481240 French.
-
Risk of Anorectal Cancer Associated with Benign Anal Inflammatory Diseases: A Retrospective Matched Cohort Study.Int J Environ Res Public Health. 2022 Jun 17;19(12):7467. doi: 10.3390/ijerph19127467. Int J Environ Res Public Health. 2022. PMID: 35742716 Free PMC article.
-
Colorectal Surgery Review for Primary Care Providers.Mo Med. 2020 Mar-Apr;117(2):154-158. Mo Med. 2020. PMID: 32308242 Free PMC article. Review.
-
Haemorrhoids, rectal prolapse, anal fissure, peri-anal fistulae and sexually transmitted diseases.Best Pract Res Clin Gastroenterol. 2009;23(4):575-92. doi: 10.1016/j.bpg.2009.04.010. Best Pract Res Clin Gastroenterol. 2009. PMID: 19647691 Review.
Cited by
-
Identifying the best therapy for chronic anal fissure.World J Gastrointest Pharmacol Ther. 2011 Apr 6;2(2):9-16. doi: 10.4292/wjgpt.v2.i2.9. World J Gastrointest Pharmacol Ther. 2011. PMID: 21577312 Free PMC article.
-
[Diagnostic yield in benign anal disease in primary care].Aten Primaria. 2009 Oct;41(10):582-3; author reply 583. doi: 10.1016/j.aprim.2009.06.011. Epub 2009 Sep 9. Aten Primaria. 2009. PMID: 19740569 Free PMC article. Spanish. No abstract available.
-
[How can we improve the care of patients with benign anorectal diseases?].Aten Primaria. 2014 Dec;46(10):582-3. doi: 10.1016/j.aprim.2014.03.011. Epub 2014 Aug 11. Aten Primaria. 2014. PMID: 25124364 Free PMC article. Spanish. No abstract available.
-
Understanding the Mechanical Forces on the Sacrum Can Help Optimize Flap-based Pilonidal Sinus Reconstruction.Plast Reconstr Surg Glob Open. 2024 Jun 19;12(6):e5923. doi: 10.1097/GOX.0000000000005923. eCollection 2024 Jun. Plast Reconstr Surg Glob Open. 2024. PMID: 38903134 Free PMC article.
References
-
- Benign anal lesions and the risk of anal cancer. N Engl J Med. 1994;331:300–302. - PubMed
-
- Lledó-Matoses S., editor., Guías clínicas de la Asociación Española de Cirujanos. Cirugía colorectal. Arán, Madrid; 2000.
-
- Latour J., Abraira V., Cabello J.B., López Sánchez J. Métodos de investigación en cardiología clínica (IV). Las mediciones clínicas en cardiología: validez y errores de medición. Rev Esp Cardiol. 1997;50:117–128. - PubMed
-
- The diagnosis and management of common anorectal disorders. Curr Probl Surg. 2004;41:586–645. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
