

Neonatal vitamin A supplementation for prevention of mortality and morbidity in infancy: systematic review of randomised controlled trials
- PMID: 19329516
- PMCID: PMC2662092
- DOI: 10.1136/bmj.b919
Neonatal vitamin A supplementation for prevention of mortality and morbidity in infancy: systematic review of randomised controlled trials
Abstract
Objective: To evaluate the effect of neonatal vitamin A supplementation on infant mortality, morbidity and early adverse effects.
Design: Systematic review, meta-analysis, and meta-regression of randomised controlled trials.
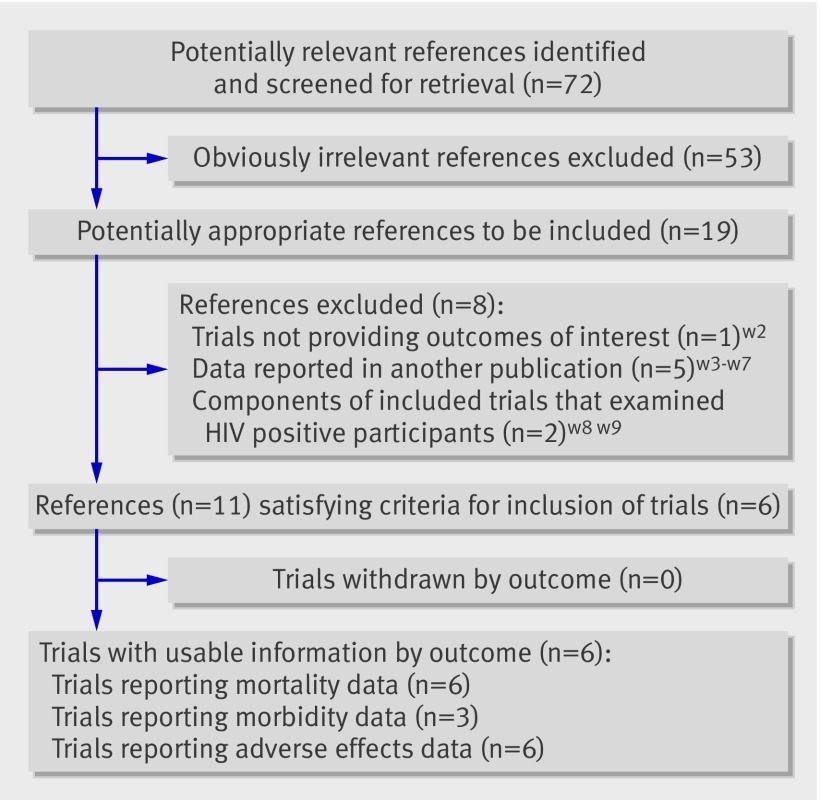
Data sources: Electronic databases and hand search of reviews; abstracts and proceedings of conferences. Review methods Randomised or quasi-randomised or cluster randomised, placebo controlled trials evaluating the effect of prophylactic, neonatal (<1 month) supplementation with synthetic vitamin A on mortality or morbidity within infancy (<1 year), and early adverse effects (</=7 days).
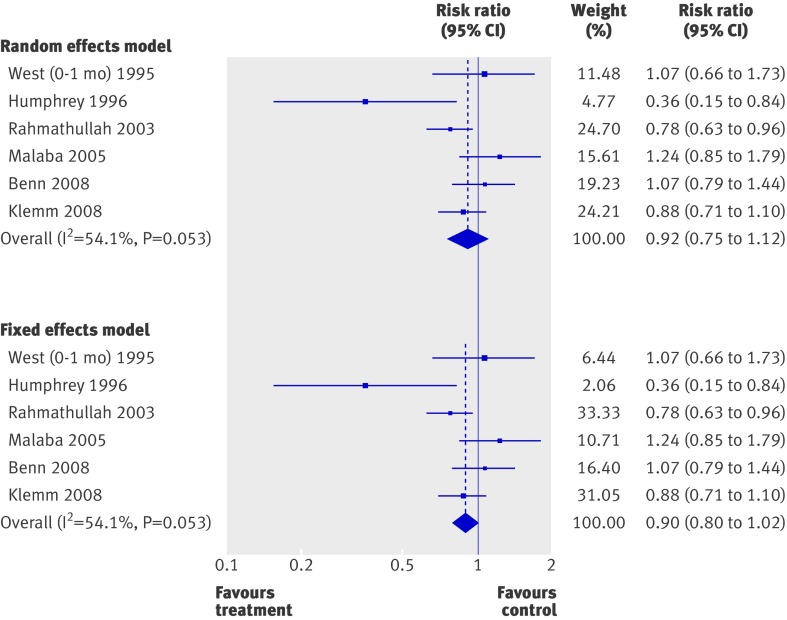
Results: The six included trials were from developing countries. There was no convincing evidence of a reduced risk of mortality during infancy (relative risk 0.92, 95% confidence interval 0.75 to 1.12, P=0.393 random effect; I(2)=54.1%) or of an increase in early adverse effects including bulging fontanelle (1.16, 0.81 to 1.65, P=0.418; I(2)=65.3%). No variable emerged as a significant predictor of mortality, but data for important risk groups (high maternal night blindness prevalence and low birth weights) were restricted. Limited data (from one to four trials) did not indicate a reduced risk of mortality during the neonatal period (0.90, 0.75 to 1.08, P=0.270; I(2)=0%), cause specific mortality, common morbidities (diarrhoea and others), and admission to hospital. There was, however, evidence of an increased risk of acute respiratory infection and a reduced risk of clinic visits.
Conclusions: There is no convincing evidence of a reduced risk of mortality and possibly morbidity or of increased early adverse effects after neonatal supplementation with vitamin A. There is thus no justification for initiating such supplementation as a public health intervention in developing countries for reducing infant mortality and morbidity.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS, Bellagio Child Survival Study Group. How many child deaths can we prevent this year? Lancet 2003;362:65-71. - PubMed
-
- Beaton GH, Martorell R, Aronson KJ, Edmonston B, McCabe G, Ross AC, et al. Effectiveness of vitamin A supplementation in the control of young child morbidity and mortality in developing countries. Geneva: ACC/SCN State of the Art Series, 1993. (Nutrition Policy Discussion Paper No 13.)
-
- Fawzi WW, Chalmers TC, Herrera MG, Mosteller F. Vitamin A supplementation and child mortality. JAMA 1993;269:898-903. - PubMed
-
- Rahmathullah L, Underwood BA, Thulsiraj RD, Milton RC, Ramaswamy K, Rahmathullah R, et al. Reduced mortality among children in Southern India receiving a small weekly dose of vitamin A. N Engl J Med 1990;323:929-35. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical