

Psychosis genetics: modeling the relationship between schizophrenia, bipolar disorder, and mixed (or "schizoaffective") psychoses
- PMID: 19329560
- PMCID: PMC2669589
- DOI: 10.1093/schbul/sbp020
Psychosis genetics: modeling the relationship between schizophrenia, bipolar disorder, and mixed (or "schizoaffective") psychoses
Abstract
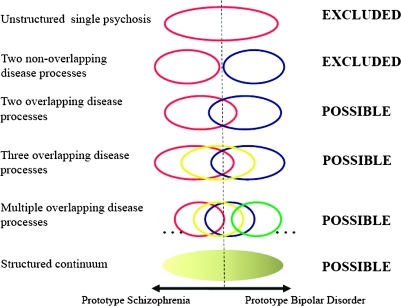
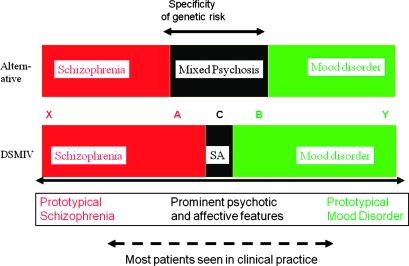
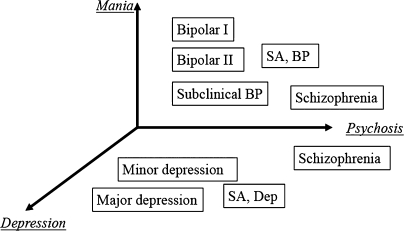
As a result of improving technologies and greatly increased sample sizes, the last 2 years has seen unprecedented advances in identification of specific genetic risk factors for psychiatric phenotypes. Strong genetic associations have been reported at common polymorphisms within ANK3 and CACNA1C in bipolar disorder and ZNF804A in schizophrenia and a relatively specific association between common variation in GABA(A) receptor genes and cases with features of both bipolar disorder and schizophrenia. Further, the occurrence of rare copy number variants (CNVs) has been shown to be increased in schizophrenia compared with controls. These emerging data provide a powerful resource for exploring the relationship between psychiatric phenotypes and can, and should, be used to inform conceptualization, classification, and diagnosis in psychiatry. It is already clear that, in general, genetic associations are not specific to one of the traditional diagnostic categories. For example, variation at ZNF804A is associated with risk of both bipolar disorder and schizophrenia, and some rare CNVs are associated with risk of autism and epilepsy as well as schizophrenia. These data are not consistent with a simple dichotomous model of functional psychosis and indicate the urgent need for moves toward approaches that (a) better represent the range of phenotypic variation seen in the clinical population and (b) reflect the underlying biological variation that gives rise to the phenotypes. We consider the implications for models of psychosis and the importance of recognizing and studying illness that has prominent affective and psychotic features. We conclude that if psychiatry is to translate the opportunities offered by new research methodologies, we must finally abandon a 19th-century dichotomy and move to a classificatory approach that is worthy of the 21st century.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
