

The Balance Evaluation Systems Test (BESTest) to differentiate balance deficits
- PMID: 19329772
- PMCID: PMC2676433
- DOI: 10.2522/ptj.20080071
The Balance Evaluation Systems Test (BESTest) to differentiate balance deficits
Abstract
Background: Current clinical balance assessment tools do not aim to help therapists identify the underlying postural control systems responsible for poor functional balance. By identifying the disordered systems underlying balance control, therapists can direct specific types of intervention for different types of balance problems.
Objective: The goal of this study was to develop a clinical balance assessment tool that aims to target 6 different balance control systems so that specific rehabilitation approaches can be designed for different balance deficits. This article presents the theoretical framework, interrater reliability, and preliminary concurrent validity for this new instrument, the Balance Evaluation Systems Test (BESTest).
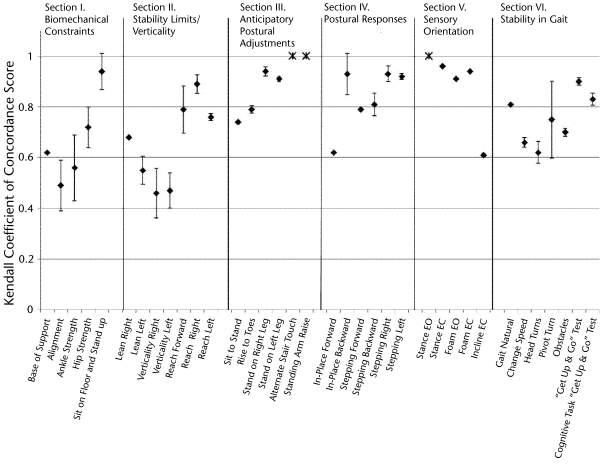
Design: The BESTest consists of 36 items, grouped into 6 systems: "Biomechanical Constraints," "Stability Limits/Verticality," "Anticipatory Postural Adjustments," "Postural Responses," "Sensory Orientation," and "Stability in Gait."
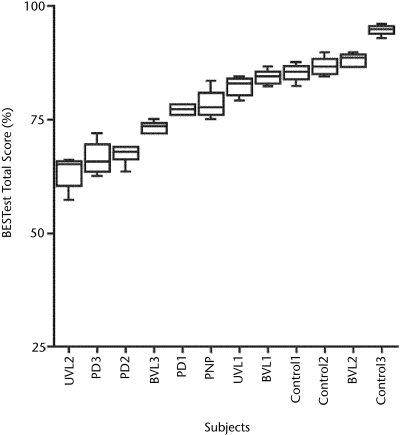
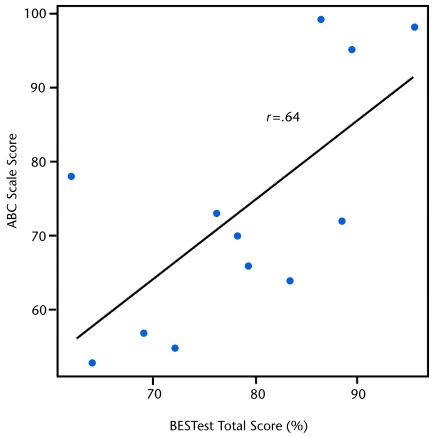
Methods: In 2 interrater trials, 22 subjects with and without balance disorders, ranging in age from 50 to 88 years, were rated concurrently on the BESTest by 19 therapists, students, and balance researchers. Concurrent validity was measured by correlation between the BESTest and balance confidence, as assessed with the Activities-specific Balance Confidence (ABC) Scale.
Results: Consistent with our theoretical framework, subjects with different diagnoses scored poorly on different sections of the BESTest. The intraclass correlation coefficient (ICC) for interrater reliability for the test as a whole was .91, with the 6 section ICCs ranging from .79 to .96. The Kendall coefficient of concordance among raters ranged from .46 to 1.00 for the 36 individual items. Concurrent validity of the correlation between the BESTest and the ABC Scale was r=.636, P<.01.
Limitations: Further testing is needed to determine whether: (1) the sections of the BESTest actually detect independent balance deficits, (2) other systems important for balance control should be added, and (3) a shorter version of the test is possible by eliminating redundant or insensitive items.
Conclusions: The BESTest is easy to learn to administer, with excellent reliability and very good validity. It is unique in allowing clinicians to determine the type of balance problems to direct specific treatments for their patients. By organizing clinical balance test items already in use, combined with new items not currently available, the BESTest is the most comprehensive clinical balance tool available and warrants further development.
Figures

References
-
- Lord SR, Clark RD, Webster IW. Physiological factors associated with falls in an elderly population. J Am Geriatr Soc. 1991;39:1194–1200. - PubMed
-
- Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39:142–148. - PubMed
-
- Berg KO, Maki BE, Williams JI, et al. Clinical and laboratory measures of postural balance in an elderly population. Arch Phys Med Rehabil. 1992;73:1073–1080. - PubMed
-
- Shumway-Cook A, Baldwin M, Polissar NL, Gruber W. Predicting the probability for falls in community-dwelling older adults. Phys Ther. 1997;77:812–819. - PubMed
-
- Shumway-Cook A, Brauer S, Woollacott MH. Predicting the probability for falls in community-dwelling older adults using the Timed “Up & Go” Test. Phys Ther. 2000;80:896–903. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
