

Case Reports
doi: 10.1590/s1807-59322009000300020.
MR imaging features of peritoneal adenomatoid mesothelioma: a case report
- PMID: 19330256
- PMCID: PMC2666464
- DOI: 10.1590/s1807-59322009000300020
Item in Clipboard
Case Reports
MR imaging features of peritoneal adenomatoid mesothelioma: a case report
Clinics (Sao Paulo).
2009.
No abstract available
Figures
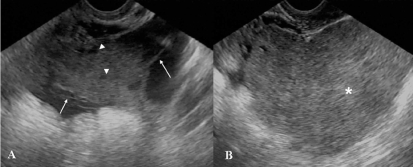
Transvaginal pelvic ultrasound images (A,B) showed a complex retrouterine mass with a homogeneous solid component (*, B) and cystic areas (arrowhead, A) intermingled with linear septa (arrow, A)
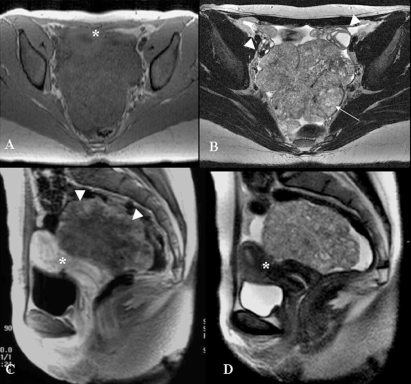
Pelvic MR exam. Axial GRE T1-weighted (A), axial TSE 512 T2-weighted (B), sagittal post-contrast GRE T1-weighted image and (D) sagittal TSE T2-weighted images. There is a large, expansive, well-delimited lesion with lobulated contours; the T1-weighted sequence shows homogeneous signal intensity predominately with a low signal, and T2-weighted sequences are heterogeneous with small high-intensity foci (arrow). The lesion dislocated the ovaries (arrowheads, B) anterolaterally and the uterus (*, A,C and D) anteriorly. After intravenous injection of paramagnetic contrast agent, there was a heterogeneous enhancement of the lesion that was more evident peripherally (arrowheads, C)

Computed tomography with no intravenous contrast agent revealed that there was no calcification within the mass (arrows)
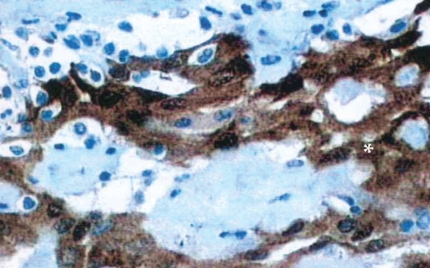
The histopathologic section shows calretinin staining for well-differentiated mesothelial cells (*), which confirms the mesothelial origin of the tumor
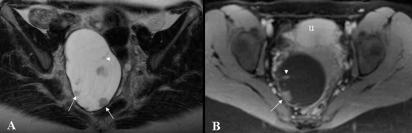
Follow-up pelvic MR exam. Axial TSE T2-weighted (A) and post-contrast axial GRE T1-weighted (B) images show a retrouterine, large, well-delimited cystic lesion with internal post-contrast-enhanced nodules (arrows) and partial septations (arrowhead). This lesion was surgically excised and histopathologically confirmed as to be a recidivate mesothelioma (u, uterus)
Similar articles
-
Diagnostic laparoscopy identifies a peritoneal adenomatoid-like mesothelioma masquerading as ovarian cancer: a case report.Eur J Gynaecol Oncol. 2014;35(1):91-4. Eur J Gynaecol Oncol. 2014. PMID: 24654472
-
[A rare primary mesothelial tumor of the peritoneum: well-differentiated papillary mesothelioma].J Radiol. 2011 Oct;92(10):936-8. doi: 10.1016/j.jradio.2011.03.027. Epub 2011 Sep 1. J Radiol. 2011. PMID: 22000617 French. No abstract available.
-
Intra-abdominal benign multicystic peritoneal mesothelioma.J Visc Surg. 2014 Apr;151(2):155-7. doi: 10.1016/j.jviscsurg.2013.12.014. Epub 2014 Jan 14. J Visc Surg. 2014. PMID: 24433857
-
[Cystic mesothelioma of the peritoneum: a clinical case report].G Chir. 1992 Jan-Feb;13(1-2):37-9. G Chir. 1992. PMID: 1581164 Review. Italian.
-
Diffuse malignant epithelial peritoneal mesothelioma in pregnancy. A case report and literature review.Eur J Gynaecol Oncol. 2004;25(1):119-22. Eur J Gynaecol Oncol. 2004. PMID: 15053080 Review.
Cited by
-
Intra-Operative Diagnosis of Benign Multicystic Peritoneal Mesothelioma: A Case Report of Rare Entity and Lessons Learned.Cureus. 2024 May 20;16(5):e60664. doi: 10.7759/cureus.60664. eCollection 2024 May. Cureus. 2024. PMID: 38899248 Free PMC article.
-
Adenomatoid mesothelioma arising from the diaphragm: a case report and review of the literature.J Med Case Rep. 2022 May 30;16(1):228. doi: 10.1186/s13256-022-03420-9. J Med Case Rep. 2022. PMID: 35637533 Free PMC article. Review.
-
Transmural peritoneal adenomatoid tumour in the ileocaecal region causing massive haemoperitoneum and low gastrointestinal bleeding: differential diagnosis with capillary haemangiomas.Ann R Coll Surg Engl. 2011 May;93(4):e3-5. doi: 10.1308/003588411X13008844892887. Ann R Coll Surg Engl. 2011. PMID: 21944783 Free PMC article.
References
-
- Hanada S, Okumura Y, Kaida K. Multicentric adenomatoid tumors involving uterus, ovary, and appendix. J Obstet Gynaecol Res. 2003;29:234–8. - PubMed
-
- Hoekman K, Tognon G, Risse EK, Bloemsma CA, Vermorken JB. Well-differentiated papillary mesothelioma of the peritoneum: a separate entity. Eur J Cancer. 1996;32A:255–8. - PubMed
-
- Wong WL, Johns TA, Herlihy WG, Martin HL. Best cases from the AFIP: multicystic mesothelioma. Radiographics. 2004;24:247–50. - PubMed
-
- Davidson B. Biological characteristics of cancers involving the serosal cavities. Crit Rev Oncog. 2007;13:189–227. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
