

Baseline risk of major bleeding in non-ST-segment-elevation myocardial infarction: the CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA Guidelines) Bleeding Score
- PMID: 19332461
- PMCID: PMC3767035
- DOI: 10.1161/CIRCULATIONAHA.108.828541
Baseline risk of major bleeding in non-ST-segment-elevation myocardial infarction: the CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA Guidelines) Bleeding Score
Abstract
Background: Treatments for non-ST-segment-elevation myocardial infarction (NSTEMI) reduce ischemic events but increase bleeding. Baseline prediction of bleeding risk can complement ischemic risk prediction for optimization of NSTEMI care; however, existing models are not well suited for this purpose.
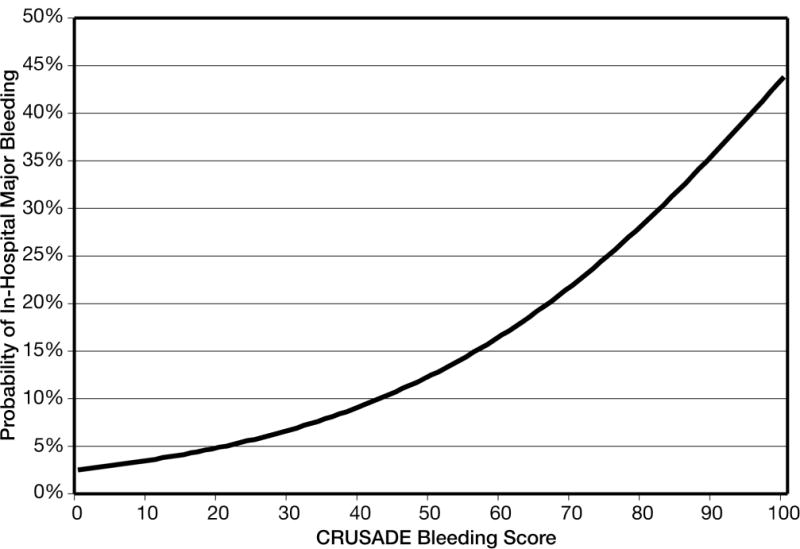
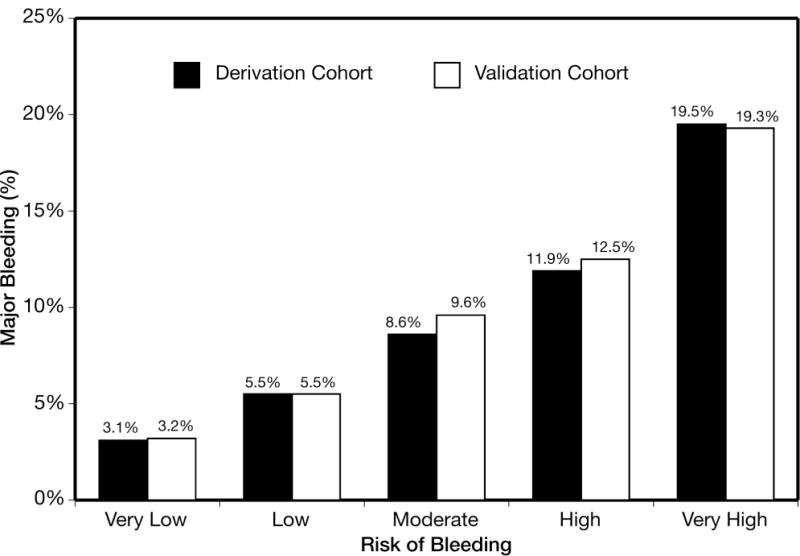
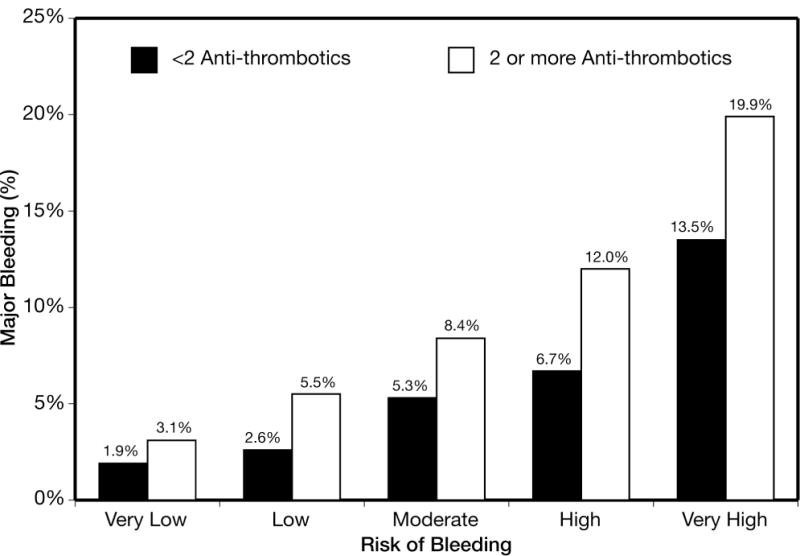
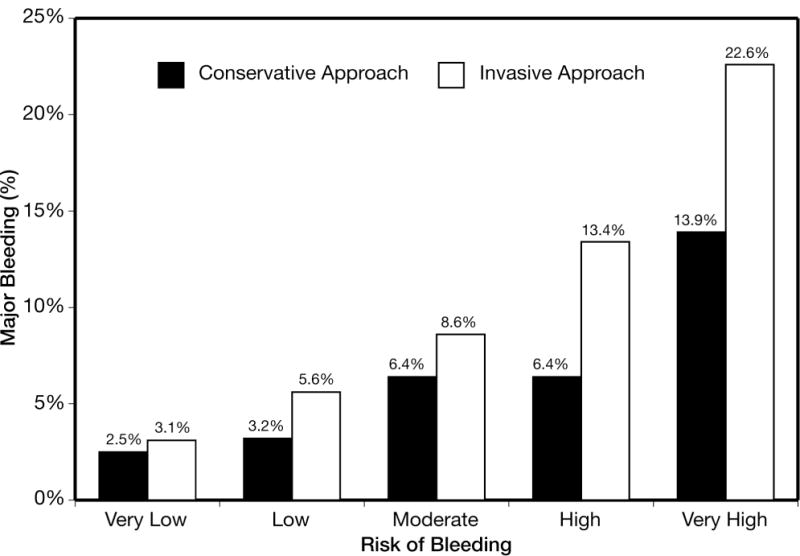
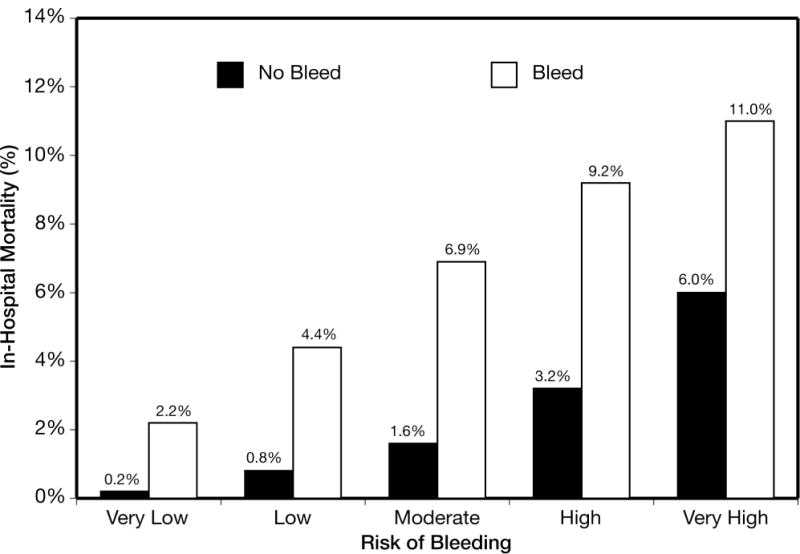
Methods and results: We developed (n=71 277) and validated (n=17 857) a model that identifies 8 independent baseline predictors of in-hospital major bleeding among community-treated NSTEMI patients enrolled in the Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines (CRUSADE) Quality Improvement Initiative. Model performance was tested by c statistics in the derivation and validation cohorts and according to postadmission treatment (ie, invasive and antithrombotic therapy). The CRUSADE bleeding score (range 1 to 100 points) was created by assignment of weighted integers that corresponded to the coefficient of each variable. The rate of major bleeding increased by bleeding risk score quintiles: 3.1% for those at very low risk (score < or = 20); 5.5% for those at low risk (score 21-30); 8.6% for those at moderate risk (score 31-40); 11.9% for those at high risk (score 41-50); and 19.5% for those at very high risk (score >50; P(trend) <0.001). The c statistics for the major bleeding model (derivation=0.72 and validation=0.71) and risk score (derivation=0.71 and validation=0.70) were similar. The c statistics for the model among treatment subgroups were as follows: > or = 2 antithrombotics=0.72; <2 antithrombotics=0.73; invasive approach=0.73; conservative approach=0.68.
Conclusions: The CRUSADE bleeding score quantifies risk for in-hospital major bleeding across all postadmission treatments, which enhances baseline risk assessment for NSTEMI care.
Conflict of interest statement
The authors have the following conflicts of interest to disclose.
Figures
Comment in
-
Stopping the hemorrhage: a new baseline bleeding score brings us a step closer for patients with non-ST-elevation myocardial infarction.Circulation. 2009 Apr 14;119(14):1846-9. doi: 10.1161/CIRCULATIONAHA.109.854281. Circulation. 2009. PMID: 19364986 No abstract available.
References
-
- Task Force for Diagnosis and Treatment of Non-ST-Segment Elevation Acute Coronary Syndromes of European Society of Cardiology. Bassand JP, Hamm CW, Ardissino D, Boersma E, Budaj A, Fernández-Avilés F, Fox KA, Hasdai D, Ohman EM, Wallentin L, Wijns W. Guidelines for the diagnosis and treatment of non–ST-segment elevation acute coronary syndromes: The Task Force for the Diagnosis and Treatment of Non–ST-Segment Elevation Acute Coronary Syndromes of the European Society of Cardiology. Eur Heart J. 2007;28:1598–1660. - PubMed
-
- Cannon CP, Weintraub WS, Demopoulos LA, Vicari R, Frey MJ, Lakkis N, Neumann FJ, Robertson DH, DeLucca PT, DiBattiste PM, Gibson CM, Braunwald E. TACTICS (Treat Angina with Aggrastat and Determine Cost of Therapy with an Invasive or Conservative Strategy)--Thrombolysis in Myocardial Infarction 18 Investigators. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001;344:1879–1887. - PubMed
-
- Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE, Jr, Chavey WE, 2nd, Fesmire FM, Hochman JS, Levin TN, Lincoff AM, Peterson ED, Theroux P, Wenger NK, Wright RS, Smith SC, Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Halperin JL, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura R, Ornato JP, Page RL, Riegel B, American College of Cardiology. American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) American College of Emergency Physicians. Society for Cardiovascular Angiography and Interventions. Society of Thoracic Surgeons. American Association of Cardiovascular and Pulmonary Rehabilitation. Society for Academic Emergency Medicine ACC/AHA 2007 guidelines for the management of patients with unstable angina/non–ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non–ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50:e1–157. - PubMed
-
- Ferguson JJ, Califf RM, Antman EM, Cohen M, Grines CL, Goodman S, Kereiakes DJ, Langer A, Mahaffey KW, Nessel CC, Armstrong PW, Avezum A, Aylward P, Becker RC, Biasucci L, Borzak S, Col J, Frey MJ, Fry E, Gulba DC, Guneri S, Gurfinkel E, Harrington R, Hochman JS, Kleiman NS, Leon MB, Lopez-Sendon JL, Pepine CJ, Ruzyllo W, Steinhubl SR, Teirstein PS, Toro-Figueroa L, White H, SYNERGY Trial Investigators Enoxaparin vs unfractionated heparin in high-risk patients with non–ST-segment elevation acute coronary syndromes managed with an intended early invasive strategy: primary results of the SYNERGY randomized trial. JAMA. 2004;292:45–54. - PubMed
-
- Stone GW, McLaurin BT, Cox DA, Bertrand ME, Lincoff AM, Moses JW, White HD, Pocock SJ, Ware JH, Feit F, Colombo A, Aylward PE, Cequier AR, Darius H, Desmet W, Ebrahimi R, Hamon M, Rasmussen LH, Rupprecht HJ, Hoekstra J, Mehran R, Ohman EM, ACUITY Investigators Bivalirudin for patients with acute coronary syndromes. N Engl J Med. 2006;355:2203–2216. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
