

Increase in activated protein C mediates acute traumatic coagulopathy in mice
- PMID: 19333141
- PMCID: PMC3574570
- DOI: 10.1097/SHK.0b013e3181a5a632
Increase in activated protein C mediates acute traumatic coagulopathy in mice
Abstract
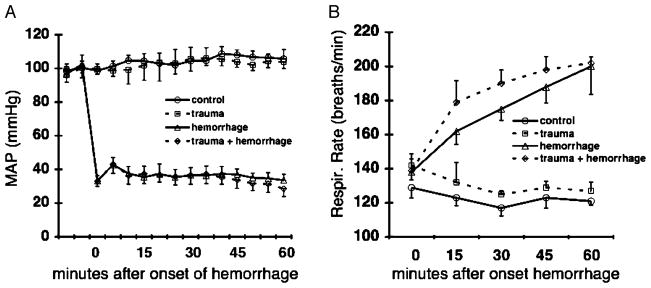
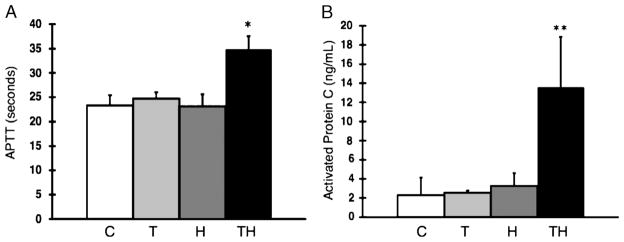
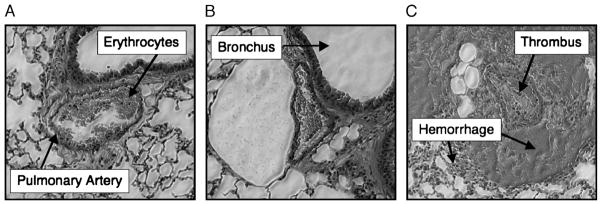
In severely injured and hypoperfused trauma patients, endogenous acute coagulopathy (EAC) is associated with an increased morbidity and mortality. Recent human data correlate this coagulopathy with activation of the protein C pathway. To examine the mechanistic role of protein C in the development of EAC, we used a mouse model of trauma and hemorrhagic shock, characterized by the combination of tissue injury and severe metabolic acidosis. Mice were subjected to one of four treatment groups: 1) C, control; 2) T, trauma (laparotomy); 3) H, hemorrhage (MAP, 35 mmHg x 60 min); 4) TH, trauma + hemorrhage. After 60 min, blood was drawn for analysis. Compared with C mice, the TH mice had a significantly elevated activated partial thromboplastin time (23.3 vs. 34.5 s) and significantly increased levels of activated protein C (aPC; 2.30 vs. 13.58 ng/mL). In contrast, T and H mice did not develop an elevated activated partial thromboplastin time or increased aPC. Selective inhibition of the anticoagulant property of aPC prevented the coagulopathy seen in response to trauma/hemorrhage (23.5 vs. 38.6 s [inhibitory vs. control monoclonal antibody]) with no impact on survival during the shock period. However, complete blockade of both the anticoagulant and cytoprotective functions of aPC caused 100% mortality within 45 min of shock, with histopathology evidence of pulmonary thrombosis and perivascular hemorrhage. These results indicate that our unique mouse model of T/H shock mimics our previous observations in trauma patients and demonstrates that EAC is mediated by the activation of the protein C pathway. In addition, the cytoprotective effect of protein C activation seems to be necessary for survival of the initial shock injury.
Figures



References
-
- World Health Organization. Injury Chart Book. Geneva, Switzerland: World Health Organization; 2002.
-
- Sauaia A, Moore FA, Moore EE, Moser KS, Brennan R, Read RA, Pons PT. Epidemiology of trauma deaths: a reassessment. J Trauma. 1995;38:185–193. - PubMed
-
- Armand R, Hess JR. Treating coagulopathy in trauma patients. Transfus Med Rev. 2003;17:223–231. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
